The Primary Patency and Fracture Rates of Self-Expandable Nitinol Stents Placed in the Popliteal Arteries, Especially in the P2 and P3 Segments, in Korean Patients
- Affiliations
-
- 1Department of Radiology, Konkuk University Hospital, Seoul 143-729, Korea.
- 2Department of Thoracic and Cardiovascular Surgery, Konkuk University Hospital, Seoul 143-729, Korea. cheehk@kuh.ac.kr
- 3Department of Surgery, Konkuk University Hospital, Seoul 143-729, Korea.
- 4Department of Orthopedic Surgery, Konkuk University Hospital, Seoul 143-729, Korea.
- KMID: 1088565
- DOI: http://doi.org/10.3348/kjr.2011.12.2.203
Abstract
OBJECTIVE
We wanted to evaluate the status of self-expandable nitinol stents implanted in the P2 and P3 segments of the popliteal artery in Korean patients.
MATERIALS AND METHODS
We retrospectively analyzed 189 consecutive patients who underwent endovascular treatment for stenoocclusive lesions in the femoropopliteal artery from July 2003 to March 2009, and 18 patients who underwent stent placement in popliteal arterial P2 and P3 segments were finally enrolled. Lesion patency was evaluated by ultrasound or CT angiography, and stent fracture was assessed by plain X-rays at 1, 3, 6 and 12 months and annually thereafter.
RESULTS
At the 1-month follow-up, stent fracture (Type 2) was seen in one limb (up to P3, 1 of 18, 6%) and it was identified in seven limbs at the 3-month follow-up (Type 2, Type 3, Type 4) (n = 1: up to P2; n = 6: P3). At the 6-month follow-up, one more fracture (Type 1) (up to P3) was noted. At the 1-year follow-up, there were no additional stent fractures. Just four limbs (up to P2) at the 2-year follow-up did not have stent fracture. The primary patency was 94%, 61% and 44% at 1, 3 and 6 months, respectively, and the group with stent implantation up to P3 had a higher fracture rate than that of the group that underwent stenting up to P2 (p < 0.05).
CONCLUSION
We suggest that stent placement up to the popliteal arterial P3 segment and over P2 in an Asian population can worsen the stent patency owing to stent fracture. It may be necessary to develop a stent design and structure for the Asian population that can resist the bending force in the knee joint.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Alloys
Angiography
Arterial Occlusive Diseases/radiography/*therapy/ultrasonography
Chi-Square Distribution
Female
Fluoroscopy
Humans
Korea
Leg/blood supply
Male
Middle Aged
Peripheral Vascular Diseases/radiography/*therapy/ultrasonography
*Popliteal Artery
Prosthesis Failure
Retrospective Studies
*Stents
Tomography, X-Ray Computed
Ultrasonography, Doppler, Color
Ultrasonography, Doppler, Duplex
Vascular Patency
Figure
-
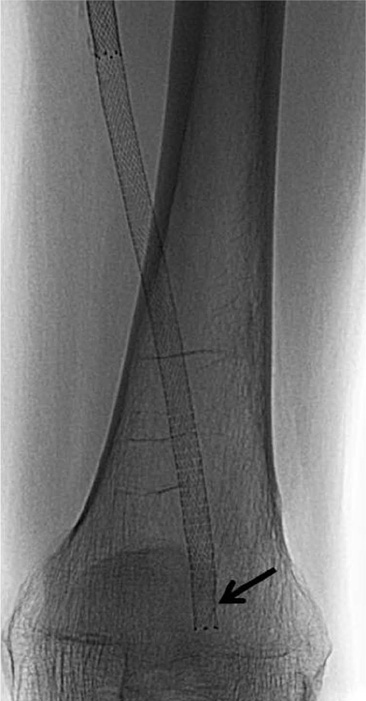
Fig. 1 66-year-old man had symptoms of severe intermittent claudication in his left leg. He had chronic total occlusion in distal superficial artery and popliteal artery. He underwent stent placement up to P2 segment for bail-out after failed balloon angioplasty. Type 1 stent fracture (arrow) was detected on fluoroscopy at 3-month follow-up.

Fig. 2 74-year-old man had diabetes with resting pain in his right foot. He had chronic total occlusion in distal superficial femoral artery and popliteal artery. He underwent stent placement up to P3 segment for bail-out after failed balloon angioplasty. At 3-month follow-up, his symptoms had recurred and type 2 stent fracture (arrows) was detected on fluoroscopy.

Fig. 3 87-year-old man had diabetes with resting pain in his right foot. He had chronic total occlusion from mid-superficial femoral artery to popliteal arterial P3 segment with massive calcifications (arrowheads). Therefore, he underwent primary stenting there. However, at 3-month follow-up, his symptoms had recurred and type 2, 3 and 4 fractures (arrows) were detected on fluoroscopy.
Reference
-
1. Dormandy JA, Rutherford RB. TASC Working Group. TransAtlantic Inter-Society Consensus (TASC). Management of peripheral arterial disease (PAD). J Vasc Surg. 2000. 31:S1–S296.2. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG, et al. Inter-society consensus for the management of peripheral arterial disease. Int Angiol. 2007. 26:81–157.3. Cejna M, Thurnher S, Illiasch H, Horvath W, Waldenberger P, Hornik K, et al. PTA versus Palmaz stent placement in femoropopliteal artery obstructions: a multicenter prospective randomized study. J Vasc Interv Radiol. 2001. 12:23–31.4. Conroy RM, Gordon IL, Tobis JM, Hiro T, Kasaoka S, Stemmer EA, et al. Angioplasty and stent placement in chronic occlusion of the superficial femoral artery: technique and results. J Vasc Interv Radiol. 2000. 11:1009–1020.5. Gordon IL, Conroy RM, Arefi M, Tobis JM, Stemmer EA, Wilson SE. Three-year outcome of endovascular treatment of superficial femoral artery occlusion. Arch Surg. 2001. 136:221–228.6. Johnston KW. Femoral and popliteal arteries: reanalysis of results of balloon angioplasty. Radiology. 1992. 183:767–771.7. Schillinger M, Sabeti S, Loewe C, Dick P, Amighi J, Mlekusch W, et al. Balloon angioplasty versus implantation of nitinol stents in the superficial femoral artery. N Engl J Med. 2006. 354:1879–1888.8. Schillinger M, Sabeti S, Dick P, Amighi J, Mlekusch W, Schlager O, et al. Sustained benefit at 2 years of primary femoropopliteal stenting compared with balloon angioplasty with optional stenting. Circulation. 2007. 115:2745–2749.9. Sabeti S, Schillinger M, Amighi J, Sherif C, Mlekusch W, Ahmadi R, et al. Primary patency of femoropopliteal arteries treated with nitinol versus stainless steel self-expanding stents: propensity score-adjusted analysis. Radiology. 2004. 232:516–521.10. Duda SH, Bosiers M, Lammer J, Scheinert D, Zeller T, Tielbeek A, et al. Sirolimus-eluting versus bare nitinol stent for obstructive superficial femoral artery disease: the SIROCCO II trial. J Vasc Interv Radiol. 2005. 16:331–338.11. Duda SH, Pusich B, Richter G, Landwehr P, Oliva VL, Tielbeek A, et al. Sirolimus-eluting stents for the treatment of obstructive superficial femoral artery disease: six-month results. Circulation. 2002. 106:1505–1509.12. Scheinert D, Scheinert S, Sax J, Piorkowski C, Braunlich S, Ulrich M, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005. 45:312–315.13. Sabeti S, Mlekusch W, Amighi J, Minar E, Schillinger M. Primary patency of long-segment self-expanding nitinol stents in the femoropopliteal arteries. J Endovasc Ther. 2005. 12:6–12.14. Strecker EP, Boos IB, Gottmann D, Vetter S, Haase W. Popliteal artery stenting using flexible tantalum stents. Cardiovasc Intervent Radiol. 2001. 24:168–175.15. Rocha-Singh KJ, Jaff MR, Crabtree TR, Bloch DA, Ansel G. Performance goals and endpoint assessments for clinical trials of femoropopliteal bare nitinol stents in patients with symptomatic peripheral arterial disease. Catheter Cardiovasc Interv. 2007. 69:910–919.16. Costanza MJ, Queral LA, Lilly MP, Finn WR. Hemodynamic outcome of endovascular therapy for TransAtlantic InterSociety Consensus type B femoropopliteal arterial occlusive lesions. J Vasc Surg. 2004. 39:343–350.17. Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005. 366:1925–1934.18. Gray BH, Sullivan TM, Childs MB, Young JR, Olin JW. High incidence of restenosis/reocclusion of stents in the percutaneous treatment of long-segment superficial femoral artery disease after suboptimal angioplasty. J Vasc Surg. 1997. 25:74–83.19. Surowiec SM, Davies MG, Eberly SW, Rhodes JM, Illig KA, Shortell CK, et al. Percutaneous angioplasty and stenting of the superficial femoral artery. J Vasc Surg. 2005. 41:269–278.20. van der Zaag ES, Legemate DA, Prins MH, Reekers JA, Jacobs MJ. Angioplasty or bypass for superficial femoral artery disease? A randomised controlled trial. Eur J Vasc Endovasc Surg. 2004. 28:132–137.21. Smouse HB, Nikanorov A, LaFlash D. Biomechanical forces in the femoropopliteal arterial segment. What happens during extremity movement and what is the effect on stenting? Endovasc Today. 2005. 4:60–66.22. Allie DE, Hebert CJ, Walker CM. Pressure-sensing guidewire analysis in RAS. Adapting this coronary-based technology to optimise "functional" renal artery revascularization could have significant clinical implications. Endovasc Today. 2004. 1:14–26.23. Iida O, Nanto S, Uematsu M, Morozumi T, Kotani J, Awata M, et al. Effect of exercise on frequency of stent fracture in the superficial femoral artery. Am J Cardiol. 2006. 98:272–274.24. Iida O, Nanto S, Uematsu M, Ikeoka K, Okamoto S, Nagata S. Influence of stent fracture on the long-term patency in the femoro-popliteal artery: experience of 4 years. JACC Cardiovasc Interv. 2009. 2:665–671.25. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007. 45:S5–S67.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early Results of Cutting Balloon Angioplasty for the Treatment of Stenoocclusive Lesions of Popliteal Arterial Segments P2 and P3
- A Dual Expandable Nitinol Stent: The Long-term Results in Patients with Malignant Gastroduodenal Strictures
- The vanishing stent: Repeated fracture and dissolution of nitinol gastric stents in a long term cancer survivor
- The challenges: Stent materials from the perspective of the manufacturer
- Self-Expandable Polytetrafluoroethylene (PTFE)-covered Nitinol Stent for the Palliative Treatment of Malignant Biliary Obstruction
