Korean J Ophthalmol.
2008 Dec;22(4):251-254. 10.3341/kjo.2008.22.4.251.
Pattern Visual Evoked Potential as a Predictor of Occlusion Therapy for Amblyopia
- Affiliations
-
- 1Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. shhan222@yumc.yonsei.ac.kr
- KMID: 1084213
- DOI: http://doi.org/10.3341/kjo.2008.22.4.251
Abstract
- PURPOSE: This study was conducted to investigate the role of the pattern visual evoked potential (pVEP) as a predictor of occlusion therapy for patients with strabismic, anisometropic, and isometropic amblyopia. The secondary aim was to compare the characteristics of pVEP between strabismic and anisometropic amblyopia. METHODS: This retrospective comparative case series included 120 patients who had received occlusion therapy or a glasses prescription for correction of strabismic, anisometropic, and isometropic amblyopia (20 patients had strabismic amblyopia, 41 patients had anisometropic amblyopia, and 59 patients had isometropic amblyopia). For each patient, the value of the P100 latency on pVEP at the time of the initial diagnosis of amblyopia was collected. Subsequently, the P100 latency was compared according to types of amblyopia. Fifty of 120 patients (7 patients with strabismic amblyopia, 21 patients with anisometropic amblyopia, and 22 patients with isometropic amblyopia) who were followed-up for longer than 6 months were divided into two groups based on the value of their P100 latency (Group 1, P100 latency 120 msec or less; Group 2, P100 latency longer than 120 msec.) The amount of visual improvement after occlusion therapy or glasses was compared between two study groups. RESULTS: The mean P100 latency was 119.7+/-25.2 msec in eyes with strabismic amblyopia and 111.9+/-17.8 msec in eyes with non-strabismic (anisometropic or isometropic) amblyopia (p=0.213). In Group 1, the mean visual improvement after occlusion therapy or glasses was 3.69+/-2.14 lines on Dr. Hahn's standard test chart; in Group 2, the mean improvement was 2.27+/-2.21 lines (p=0.023). CONCLUSIONS: The P100 latency on pVEP at the time of initial diagnosis was significantly related to the visual improvement after occlusion therapy or glasses in patients with strabismic, anisometropic, and isometropic amblyopia. Therefore, it was presumed that patients with a delayed P100 latency might have less visual improvement after occlusion therapy or glasses. In addition, there was no apparent difference in P100 latency between patients with strabismic and non-strabismic (anisometropic or isometropic) amblyopia.
Keyword
MeSH Terms
Figure
-
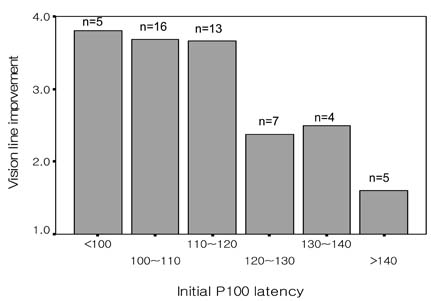
Fig. 1 Vision improvement according to initial P100 latency. In patients with a P100 latency shorter than 120 msec, the vision was improved by 3.69±2.14 lines on Dr. Hahn's standard test chart, and in patients with a P100 latency longer than 120 msec, the vision was improved by 2.27±2.21 lines (p=0.023).
Cited by 1 articles
-
Pattern VEP in Adult Amblyopic Patients Requested From Military Service
Woong Sun Yoo, Yeon Jung Park, Ji Myong Yoo
J Korean Ophthalmol Soc. 2010;51(10):1392-1397. doi: 10.3341/jkos.2010.51.10.1392.
Reference
-
1. Iliakis E, Moschos M, Hontos N, et al. The prognostic value of visual evoked response latency in the treatment of amblyopia caused by strabismus. Doc Ophthalmol. 1996-1997. 92:223–228.2. Ridder WH 3rd, Rouse MW. Predicting potential acuities in amblyopes: predicting post-therapy acuity in amblyopse. Doc Ophthalmol. 2007. 114:135–145.3. Oner A, Coskun M, Evereklioglu C, Dogan H. Pattern VEP is a useful technique in monitoring the effectiveness of occlusion therapy in amblyopic eyes under occlusion therapy. Doc Ophthalmol. 2004. 109:223–227.4. Johansson B, Jakobsson P. Fourier analysis steady-state VEPs in pre-school children with and without normal binocularity. Doc Ophthalmol. 2006. 112:13–22.5. Simon JW, Siegfried JB, Mills MD, et al. A new visual evoked potential system for vision screening in infants and young children. J AAPOS. 2004. 8:549–554.6. Ohn YH, Katsumi O, Matsui Y, et al. Snellen visual acuity versus pattern reversal visual-evoked response acuity in clinical applications. Ophthalmic Res. 1994. 26:240–252.7. Jenkins TC, Douthwaite WA, Peedle JE. The VER as a predictor of normal visual acuity in the adult human eye. Ophthalmic Physiol Opt. 1985. 5:441–449.8. Kubová Z, Kuba M, Juran J, Blakemore C. Is the motion system relatively spared in amblyopia? Evidence from cortical evoked responses. Vision Res. 1996. 36:181–190.9. Palmer EZ. Amblyopia. Prepared by the American Academy of Ophthalmology, Quality of Care Committee. Pediatric Ophthalmology Panel. 1992. 1–24.10. von Noorden GK. Amblyopia. A multidisciplinary approach. Invest Ophthalmol Vis Sci. 1985. 26:1704.11. Simons K. Preschool vision screening: rationale, methodology and outcome. Surv Ophthalmol. 1996. 41:3–30.12. Attebo K, Mitchell P, Cumming R, et al. Prevelance and causes of amblyopia in an adult population. Ophthalmology. 1998. 105:154–159.13. Sokol S. Pattern visual evoked potentials: their use in pediatric ophthalmology. Int Ophthalmol Clin. 1980. 20:251–268.14. Arden GB, Barnard WM, Mushin AS. Visually evoked responses in amblyopia. Br J Ophthalmol. 1974. 58:183–192.15. Sokol S. Abnormal evoked potential latencies in amblyopia. Br J Ophthalmol. 1983. 67:310–314.16. Yin ZQ, Fang QX. The simultaneously recorded of PERG and PVEP in amblyopic children. Chin J Ophthalmol. 1989. 5:312–315.17. Yu M, Brown B, Edwards MH. Investigation of multifocal visual evoked potential in anisometropic and esotropic amblyopes. Invest Ophthalmol Vis Sci. 1998. 39:2033–2040.18. Wildberger H. The relationship between visual evoked potentials (VEPs) and visual acuity in amblyopia. Docum Ophthal Proc Series. 1982. 31:385–390.19. Wilcox LM Jr, Sokol S. Changes in the binocular fixation pattern and the visually evoked potential in the treatment of esotropia with amblyopia. Ophthalmology. 1980. 87:1273–1281.20. Galloway NR, Barber C. Transient visual evoked potential monitoring of disuse amnblyopia. Docum Ophthal Proc Series. 1982. 31:377–384.21. Harter MR, White CT. Evoked cortical response to checkerboard patterns: effect of check-size as a function of visual acuity. Electroencephalogr Clin Neurophysiol. 1970. 28:48–54.22. Sokol S, Bloom B. Visually evoked cortical responses of amblyopes to a spatially alternating stimulus. Invest Ophthalmol. 1973. 12:936–939.23. Howe JW, Mitchell KW, Robson C. Electrophysiological assessment of visual acuity. Trans Ophthalmol Soc U K. 1981. 101:105–108.24. Fagan JE Jr, Yolton RL. Theoretical reliability of visual evoked response-based acuity determinations. Am J Optom Physiol Opt. 1985. 62:95–99.25. Friendly DS, Weiss IP, Barnet AB, et al. Pattern-reversal visual-evoked potentials in the diagnosis of amblyopia in children. Am J Ophthalmol. 1986. 102:329–339.26. Jenkins TC, Douthwaite WA. An objective VER assessment of visual acuity compared with subjective measures. Am J Optom Physiol Opt. 1988. 65:957–961.27. Steele M, Seiple WH, Carr RE, Klug R. The clinical utility of visual-evoked potential acuity testing. Am J Ophthalmol. 1989. 108:572–577.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Change of Multifocal Visual Evoked Potential in Unilateral Anisometropic Amblyopia before and after Occlusion Treatment
- Effect of Occlusion Therapy and Change of VEP in Amblyopia
- Efficacy of Occlusion Therapy in Amblyopia: Type, Depth and Timing of Amblyopia
- Visual Evoked Potential Study in Amblyopia and Normal Groups
- Pattern-VEP in Child Amblyopia
