Optic Disc Pit with Peripapillary Retinoschisis Presenting as a Localized Retinal Nerve Fiber Layer Defect
- Affiliations
-
- 1Department of Ophthalmology, Hanyang University College of Medicine, Seoul, Korea. KBUhm@hanyang.ac.kr
- KMID: 1031196
- DOI: http://doi.org/10.3341/kjo.2011.25.6.455
Abstract
- A 59-year-old woman was referred to our clinic for a glaucoma evaluation. The visual acuity and intraocular pressure were normal in both eyes. However, red-free fundus photography in the left eye showed a superotemporal wedge-shaped retinal nerve fiber layer defect, and visual field testing showed a corresponding partial arcuate scotoma. In an optical coherence tomography examination, the macula was flat, but an arcuate-shaped peripapillary retinoschisis was found. Further, the retinoschisis seemed to be connected with a superotemporal optic pit shown in a disc photograph. After 3 months of a topical prostaglandin analogue medication, the intraocular pressure in the retinoschisis eye was lowered from 14 to 10 mmHg and the peripapillary retinoschisis was almost resolved. We report a rare case of an optic disc pit with peripapillary retinoschisis presenting as a localized retinal nerve fiber layer defect.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Disc photography showing a round, gray, superotemporal optic disc pit (black arrow) in the left eye. (B) Red-free fundus photography. The superotemporal wedge-shaped retinal nerve fiber layer defect is shown (white arrow). (C) An infrared laser ophthalmoscope image shows the optic disc pit more clearly (white arrow). (D) After 3 months of a topical prostaglandin analogue medication, the retinal nerve fiber layer defect seems to have decreased (white arrow).
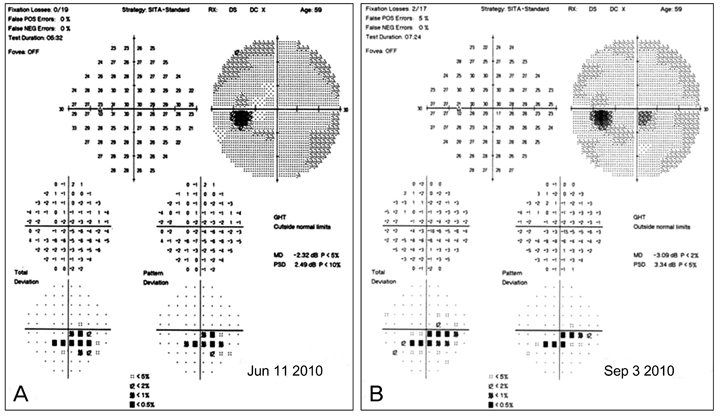
Fig. 2 (A) Humphrey visual field testing in the left eye showed the inferior partial arcuate scotoma corresponding with the superotemporal retinal nerve fiber layer defect. (B) After 3 months of topical prostaglandin analogue medication, there was no change in the results of visual field testing.
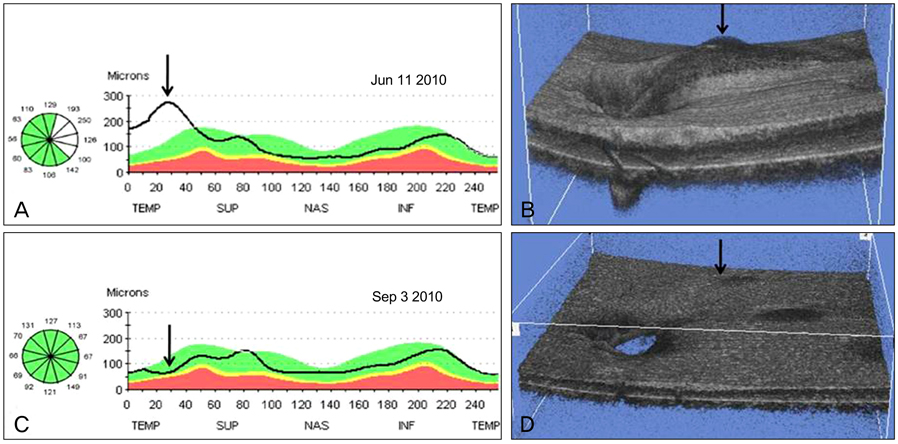
Fig. 3 (A) An optical coherence tomography retinal nerve fiber layer scan in the left eye demonstrated retinal nerve fiber layer (RNFL) thickening of the superotemporal region (arrow) rather than RNFL thinning. (B) Optical coherence tomography (OCT) 3-D reconstruction imaging shows superotemporal peripapillary retinoschisis as a 3-D (arrow). (C) After 3 months of topical prostaglandin analogue medication, an OCT RNFL scan revealed a decrease in RNFL (arrow). (D) OCT 3-D reconstruction imaging shows the decreased peripapillary retinoschisis (arrow). TEMP=temporal; SUP = superior; NAS = nasal; INF = inferior.
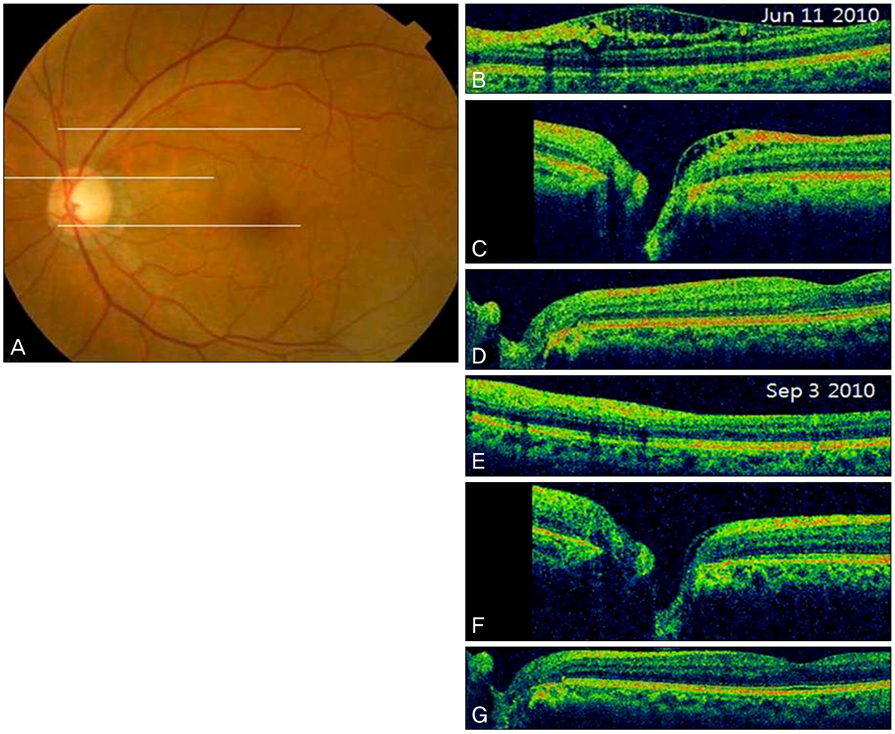
Fig. 4 (A) Fundus photography. (B) Optical coherence tomography (OCT) slice at the superotemporal region from the optic disc (upper white line in A) shows inner retinal schisis cavities. (C) OCT slice at the level of the superior part of the optic disc and some part of the macula (middle white line in A) shows the peripapillary retinoschisis, not extending to the macula. (D) OCT slice at the level of the inferior part of the optic disc and the fovea (lower white line in A) shows that there is no retinoschisis in the papillomacular retinal region. (E,F,G) After 3 months of topical prostaglandin analogue medication, the OCT scan shows that the peripapillary retinoschisis is partially resolved.
Cited by 1 articles
-
Peripapillary Retinoschisis in Non-Glaucomatous Eyes
Sun Young Jin, Mi Ryoung Song, Min Kyung Kim, Young Hoon Hwang
J Korean Ophthalmol Soc. 2015;56(1):80-85. doi: 10.3341/jkos.2015.56.1.80.
Reference
-
1. Kranenburg EW. Crater-like holes in the optic disc and central serous retinopathy. Arch Ophthalmol. 1960. 64:912–924.2. Brown GC, Shields JA, Goldberg RE. Congenital pits of the optic nerve head. II. Clinical studies in humans. Ophthalmology. 1980. 87:51–65.3. Krivoy D, Gentile R, Liebmann JM, et al. Imaging congenital optic disc pits and associated maculopathy using optical coherence tomography. Arch Ophthalmol. 1996. 114:165–170.4. Sobol WM, Blodi CF, Folk JC, Weingeist TA. Long-term visual outcome in patients with optic nerve pit and serous retinal detachment of the macula. Ophthalmology. 1990. 97:1539–1542.5. Ryan SJ. Retina. 2006. 2:4th ed. Philadelphia: Mosby Elsevier;1883.6. Brodsky MC. Congenital optic disk anomalies. Surv Ophthalmol. 1994. 39:89–112.7. Lincoff H, Lopez R, Kreissig I, et al. Retinoschisis associated with optic nerve pits. Arch Ophthalmol. 1988. 106:61–67.8. Lincoff H, Schiff W, Krivoy D, Ritch R. Optic coherence tomography of optic disk pit maculopathy. Am J Ophthalmol. 1996. 122:264–266.9. Radius RL, Maumenee AE, Green WR. Pit-like changes of the optic nerve head in open-angle glaucoma. Br J Ophthalmol. 1978. 62:389–393.10. Javitt JC, Spaeth GL, Katz LJ, et al. Acquired pits of the optic nerve. Increased prevalence in patients with low-tension glaucoma. Ophthalmology. 1990. 97:1038–1043.11. Nduaguba C, Ugurlu S, Caprioli J. Acquired pits of the optic nerve in glaucoma: prevalence and associated visual field loss. Acta Ophthalmol Scand. 1998. 76:273–277.12. Ugurlu S, Weitzman M, Nduaguba C, Caprioli J. Acquired pit of the optic nerve: a risk factor for progression of glaucoma. Am J Ophthalmol. 1998. 125:457–464.13. Healey PR, Mitchell P. The prevalence of optic disc pits and their relationship to glaucoma. J Glaucoma. 2008. 17:11–14.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Retinal Herniation through Peripapillary Pit Resulting in Retinal Nerve Fiber Layer Defect
- A Comparison of Retinal Thickness Changes According to Initial Optic Disc Edema in Optic Neuritis Patients
- A Case of Optic Disc Pit
- Reproducibility of Retinal Nerve Fiber Layer Thickness Evaluation by Nerve Fiber Analyzer
- Two Cases of Topless Optic Disc Syndrome
