Pyogenic L4-5 Spondylitis Managed with Percutaneous Drainage Followed by Posterior Lumbar Interbody Fusion: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Chungbuk National University, Cheongju, Korea. ymkim@med.chungbuk.ac.kr
Abstract
-
STUDY DESIGN: A case report and review of literature
OBJECTIVE
Mostly operative treatment for pyogenic spondylits has been performed via anterior approach, which is often followed by greater morbidity and late sequelae. Efficacy of percutaneous drainage and posterior lumbar interbody fusion (PLIF), which are increasingly applied with favorable results, as an alternative of anterior surgery was investigated. MATERIAL AND METHOD: A case of pyogenic L4-5 spondylitis with psoas abscess but without neurologic deficit in a 66-year old lady was reviewed. Percutaneous drainage under fluoroscopic guide was performed. 7 weeks later, curettage of disc space and posterior lumbar interbody fusion using autogeous graft was performed to get rid of dead space and achieve stability. Administration of antimicrobial agents followed.
RESULTS
Infection was controlled successfully. Clinical features including ambulatory function improved. Solid fusion was achieved. SUMMARY: In treating pyogenic spondylitis with moderate abscess, percutaneous drainage and posterior lumbar interbody fusion seemed to be one of alternatives of anterior surgery.
Keyword
MeSH Terms
Figure
-
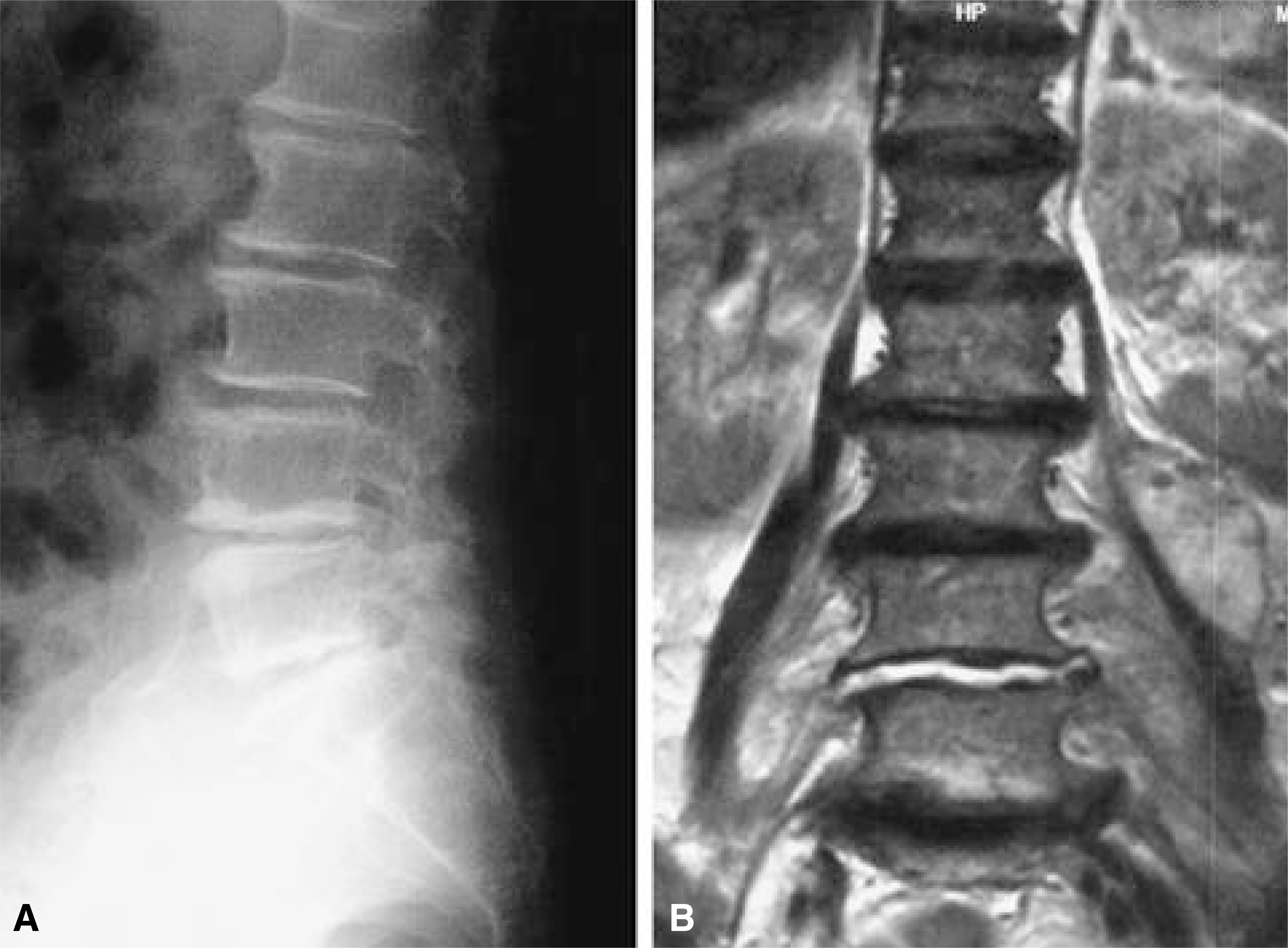
Fig. 1 A. Initial lateral radiographs shows mild narrowing of L4-5 disc space and subchondral sclerosis adjacent to the end plates. Fig. 1-B. Initial T2-weighted coronal image reveals high signal intensity in L4-5 disc space and moderate bilateral psoas abscess without significant bone destruction.

Fig. 2-A. Lateral X-ray at 7 weeks post-PCD shows progression of bony destruction. Fig. 2-B. Preoperative T2-weighted sagittal image reveals expanded intervertebral dead space filled with fluid, L4-5. Fig. 2-C. T2 coronal image shows widened dead space and irregular bony destruction.

Fig. 3-A. After thorough curettage of intervertebral dead space and copious irrigation, transpedicular screws were inserted. Fig. 3-B. Continuous suction drainage for 3 weeks followed.

Fig. 4-A. Complete solid fusion at postoperative 1 year. Fig. 3-B. Lateral X-ray shows good sagittal alignment.
Reference
-
1). Chung YG, Ha KY. Adherence and biofilm formation of Staphylococcus epidermidis and Mycobacterium tuberculosis on spinal implant. J Kor Spine Surg. 6(1):47–56. 1999.2). Chung YK, Kim SW, Han HM, Lee EJ, Choi SJ, Chang JD. The results of the surgical treatment using posterior spinal instrumentation for tuberculous spondylitis. J Kor Spine Surg. 6(1):81–88. 1999.3). Conterton JW, Irvin RT, Cheng KJ. The bacterial glycocalyx in nature and disease. Ann Rev Microbial. 35:299–324. 1981.4). Eysel P, Hopf Ch, Vegel I, Rompe JD. Primary sta -ble anterior instrumentation or dorsoventral spondylodesis in spondylodiscitis? Eur Spine J. 6:152–157. 1997.5). Jeanneret B, Magerl F. Treatment of osteomyelitis of the spine using percutaneous suction/irrigation and percutaneous external spine fixation. J Spinal Disord. 7(3):185–205. 1994.6). Kim DJ, Wang JM. The posterior instrumentation using compressive laminar hooks combined with anterior interbody fusion for the treatment of tuberculous spondylitis in the lower lumbar spine. J Kor Spine Surg. 6(1):8–14. 1999.7). Krödel A, Krüger A, Lohscheidt K, Pfahler M, Re-fior HJ. Anterior debridement fusion and extrafocal stabilization in the treatment of osteomyelitis of the spine. J Spinal Disord. 2:17–26. 1999.8). Kwon KH, Park JH, Chae IJ. Percutaneous drainage and irrigation in pyogenic vertebral osteomyelitis. J Kor Spine Surg. 5(1):122–128. 1998.9). Nagata K, Ohashi T, Ariyoshi M, Sonoda K, Imoto H, Inoue A. Percutaneous suction aspiration and drainage for pyogenic spondylitis. Spine. 23(14):1600–1606. 1998.
Article10). Oga M, Arizono T, Takasita M, Sugioka Y. Evaluation of the risk of instrumentation as a foreign body in spinal tuberculosis. Spine. 18:1890–1894. 1993.
Article11). Park JT, Ahn GY, Kim HG, Seong YW. The results of anterior fusion with anterior instrumentation in spinal tuberculosis(preliminary study). J Kor Spine Surg. 3(2):217–224. 1996.12). Park WW, Park YS, Cheon SJ, Jung JY. Posterior lumbar interbody fusion in the pyogenic discitis. J Kor Spine Surg. 8(1):39–45. 2001.
Article13). Safran O, Rand N, Kaplan L, Sagiv S, Floman Y. Sequential or simultaneous sameday anterior decompression and posterior stabilization in the management of vertebral osteomyelitis of the lumbar spine. Spine. 23:1885–90. 1998.
Article14). Yu W, Siu C, Wing PC, Schweigel JF, Jetha N. Percutaneous suction aspiration for osteomyelitis. Report of two cases. Spine. 16:198–202. 1991.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pyogenic L4-5 Spondylitis Managed with Percutaneous Drainage Followed by Posterior Lumbar Interbody Fusion: A Case Report
- Management of Lumbar Pyogenic Spondylitis with Posterior Decompression and Interbody Fusion Using Transpedicular Screws
- Posterior Lumbar Interbody Fusion
- Percutaneous Transpedicular Interbody Fusion Technique in Percutaneous Pedicle Screw Stabilization for Pseudoarthrosis Following Pyogenic Spondylitis
- Anterior Lumbar Interbody Fusion with Percutaneous Pedicle Screw Fixation for the Treatment of Postoperative Pyogenic Spondylodiscitis
