MRI of the Breast for the Detection and Assessment of the Size of Ductal Carcinoma in Situ
- Affiliations
-
- 1Department of Radiology, College of Medicine Seoul National University and The Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea. moonwk@radcom.snu.ac.kr
- 2Department of Pathology, College of Medicine Seoul National University and The Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea.
- 3Department of Radiology, Boramae Municipal Hospital, Seoul, Korea.
- KMID: 753863
- DOI: http://doi.org/10.3348/kjr.2007.8.1.32
Abstract
OBJECTIVE
The aim of the study was to compare the accuracy of magnetic resonance imaging (MRI) and mammography for the detection and assessment of the size of ductal carcinoma in situ (DCIS). MATERIALS AND METHODS: The preoperative contrast-enhanced MRI and mammography were analyzed in respect of the detection and assessment of the size of DCIS in 72 patients (age range: 30-67 years, mean age: 47 years). The MRI and mammographic measurements were compared with the histopathologic size with using the Pearson's correlation coefficients and the Mann-Whitney u test. We evaluated whether the breast density, the tumor nuclear grade, the presence of comedo necrosis and microinvasion influenced the MRI and mammographic size estimates by using the chi-square test. RESULTS: Of the 72 DCIS lesions, 68 (94%) were detected by MRI and 62 (86%) were detected by mammography. Overall, the Pearson's correlation of the size between MRI and histopathology was 0.786 versus 0.633 between mammography and histopathology (p < 0.001). MRI underestimated the size by more than 1 cm (including false negative examination) in 12 patients (17%), was accurate in 52 patients (72%) and overestimated the size by more than 1 cm in eight patients (11%) whereas mammography underestimated the size in 25 patients (35%), was accurate in 31 patients (43%) and overestimated the size in 16 patients (22%). The MRI, but not the mammography, showed significant correlation for the assessment of the size of tumor in noncomedo DCIS (p < 0.001 vs p = 0.060). The assessment of tumor size by MRI was affected by the nuclear grade (p = 0.008) and the presence of comedo necrosis (p = 0.029), but not by the breast density (p = 0.747) or microinvasion (p = 0.093). CONCLUSION: MRI was more accurate for the detection and assessment of the size of DCIS than mammography.
MeSH Terms
Figure
-
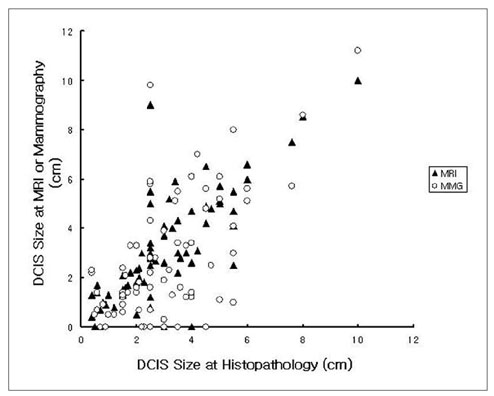
Fig. 1 Graph showing the correlation between the histopathologically determined DCIS size and the corresponding DCIS size as measured by MRI and mammography. The mean absolute difference in the size between imaging and histopathology was 0.8 cm (0-6.5 cm) by MRI and 1.5 cm (0-7.3 cm) by mammography. DCIS = Ductal carinoma in situ, MRI = Magnetic resonance imaging, MMG = Mammography.
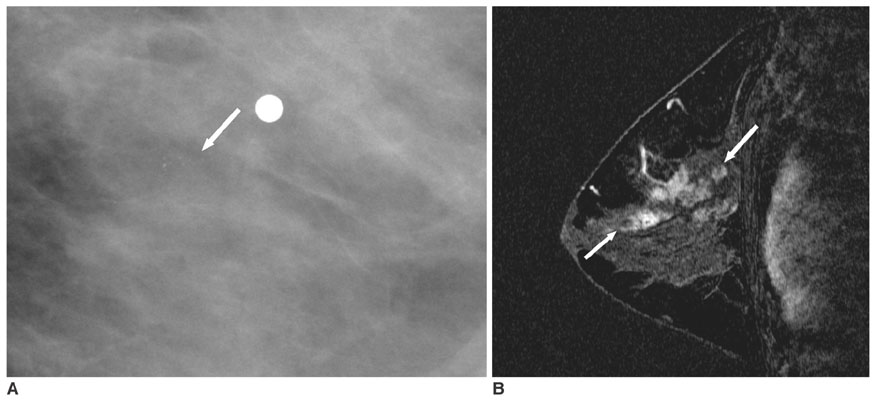
Fig. 2 A 45-year-old woman with a 5 cm high grade, comedo type DCIS, which was more accurately assessed by MRI than by mammography. A. Spot-magnification mediolateral oblique mammogram shows a 1.1 cm cluster of the pleomorphic microcalcifications (arrow) in the left breast. The metallic marker is on the palpable area. B. Dynamic contrast-enhanced sagittal subtraction MR image shows a 5 cm sized, segmentally distributed, heterogeneous enhancing lesion (arrows) in the left breast.
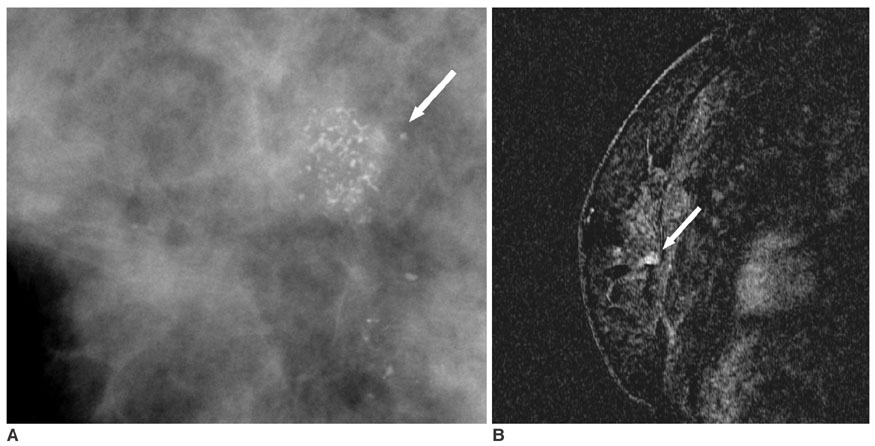
Fig. 3 A 43-year-old woman with a 2 cm high grade, comedo type DCIS, which was more accurately assessed by mammography than by MRI. A. Spot-magnification mediolateral oblique mammogram shows a 1.4 cm segmental distribution of the pleomorphic microcalcifications (arrow) in the right breast. B. Dynamic contrast-enhanced sagittal subtraction MR image shows a 0.5 cm sized, irregular enhancing lesion (arrow) in the right breast.
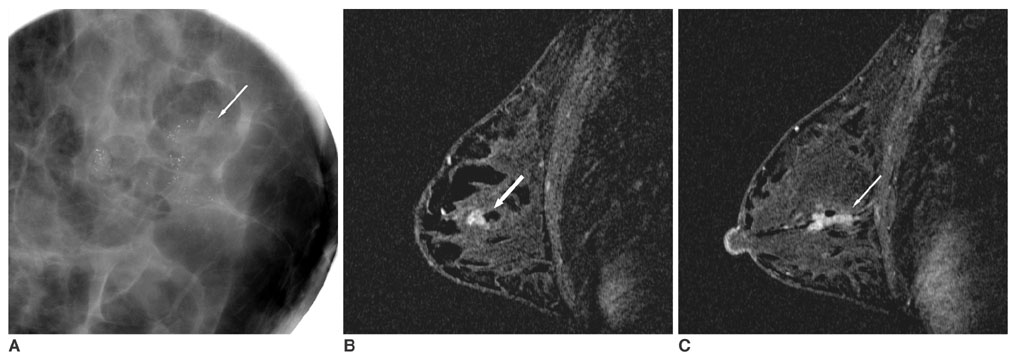
Fig. 4 A 33-year-old woman with a 2.7 cm high grade, comedo type DCIS, which was accurately assessed by both MRI and mammography. A. Spot-magnification mediolateral oblique mammogram shows a 2.7 cm segmental distribution of the pleomorphic microcalcifications (arrow) in the left breast. B, C. Dynamic contrast-enhanced sagittal subtraction MR images shows a 2.7 cm sized, clumped ductal enhancement (arrows) in the left breast.
Cited by 3 articles
-
The Role and Significance of Preoperative Breast MRI in the Setting of Breast Cancer
Jun Woo Jin, Cha Kyong Yom, Min Young Koo, Byung In Moon, Kook Jin Choi, Hye Young Choi
J Breast Cancer. 2008;11(3):146-150. doi: 10.4048/jbc.2008.11.3.146.A Comparative Study between the Preoperative Diagnostic Tumor Size and the Postoperative Pathologic Tumor Size in Patients with Breast Tumors
Ki-Tae Hwang, Hyeyoung Kim, Jung Kee Chung, In Mok Jung, Seung Chul Heo, Young Joon Ahn, Hye Seong Ahn, Joo Hee Cha, Se-Yeong Chung, Mee Soo Chang, Dong-Young Noh
J Breast Cancer. 2010;13(2):187-197. doi: 10.4048/jbc.2010.13.2.187.Conventional Galactography and MR Contrast Galactography for Diagnosing Nipple Discharge: Preliminary Results
Cüneyt Yücesoy, Emine Öztürk, Yusuf Özer, Tahsin Edgüer, Baki Hekimoglu
Korean J Radiol. 2008;9(5):426-431. doi: 10.3348/kjr.2008.9.5.426.
Reference
-
1. Dershaw DD, Abramson A, Kinne DW. Ductal carcinoma in situ: mammographic findings and clinical implications. Radiology. 1989. 170:411–415.2. Stomper PC, Connolly JL, Meyer JE, Harris JR. Clinically occult ductal carcinoma in situ detected with mammography: analysis of 100 cases with radiologic-pathologic correlation. Radiology. 1989. 172:235–241.3. Ikeda DM, Andersson I. Ductal carcinoma in situ (DCIS): atypical mammographic appearances. Radiology. 1989. 172:661–666.4. Silverstein MJ. Ductal carcinoma in situ (DCIS) of the breast: diagnostic and therapeutic controversies. J Am Coll Surg. 2001. 192:196–214.5. Orel SG, Schnall MD, LiVolsi VA, Troupin RH. Suspicious breast lesions: MR imaging with radiologic-pathologic correlation. Radiology. 1994. 190:485–493.6. Soderstrom CE, Harms SE, Copit DS, Evans WP, Savino DA, Krakos PA, et al. Three-dimensional RODEO breast MR imaging of lesions containing ductal carcinoma in situ. Radiology. 1996. 201:427–432.7. Kristoffersen Wiberg M, Aspelin P, Sylvan M, Bone B. Comparison of lesion size estimated by dynamic MR imaging, mammography and histopathology in breast neoplasms. Eur Radiol. 2003. 13:1207–1212.8. Mumtaz H, Hall-Craggs MA, Davidson T, Walmsley K, Thurell W, Kissin MW, et al. Staging of symptomatic primary breast cancer with MR imaging. AJR Am J Roentgenol. 1997. 169:417–424.9. Morris EA, Liberman L, Ballon DJ, Robson M, Abramson AF, Heerdt A, et al. MRI of occult breast carcinoma in a high-risk population. AJR Am J Roentgenol. 2003. 181:619–626.10. Hata T, Takahashi H, Watanabe K, Takahashi K, Taguchi K, Itoh T, et al. Magnetic resonance imaging for preoperative evaluation of breast cancer: a comparative study with mammography and ultrasonography. J Am Coll Surg. 2004. 198:190–197.11. Van Goethem M, Schelfout K, Dijckmans L, Van Der Auwera JC, Weyler J, Verslegers I, et al. MR mammography in the preoperative staging of breast cancer in patients with dense breast tissue: comparison with mammography and ultrasound. Eur Radiol. 2004. 14:809–816.12. Boetes C, Mus RD, Holland R, Barentsz JO, Strijk SP, Wobbes T, et al. Breast tumors: comparative accuracy of MR imaging relative to mammography and US for demonstrating extent. Radiology. 1995. 197:743–747.13. Gilles R, Zafrani B, Guinebretiere JM, Meunier M, Lucidarme O, Tardivon AA, et al. Ductal carcinoma in situ: MR imaging-histopathologic correlation. Radiology. 1995. 196:415–419.14. Heywang-Kobrunner SH. Contrast-enhanced magnetic resonance imaging of the breast. Invest Radiol. 1994. 29:94–104.15. American College of Radiology. Breast imaging reporting and data system (BI-RADS). 2003. Reston, Va: American College of Radiology.16. Boetes C, Strijk SP, Holland R, Barentsz JO, Van Der Sluis RF, Ruijs JH. False-negative MR imaging of malignant breast tumors. Eur Radiol. 1997. 7:1231–1234.17. Bluemke DA, Gatsonis CA, Chen MH, DeAngelis GA, DeBruhl N, Harms S, et al. Magnetic resonance imaging of the breast prior to biopsy. JAMA. 2004. 292:2735–2742.18. Folkman J. What is the evidence that tumors are angiogenesis dependent? J Natl Cancer Inst. 1990. 82:4–6.19. Guidi AJ, Fischer L, Harris JR, Schnitt SJ. Microvessel density and distribution in ductal carcinoma in situ of breast. J Natl Cancer Inst. 1994. 86:614–619.20. Neubauer H, Li M, Kuehne-Heid R, Schneider A, Kaiser WA. High grade and non-high grade ductal carcinoma in situ on dynamic MR mammography: characteristic findings for signal increased and morphological pattern of enhancement. Br J Radiol. 2003. 76:3–12.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Unusual Presentation of Extensive Ductal Carcinoma in Situ Accompanying Invasive Ductal Carcinoma on MRI: A Case Report
- Invasive Lobular Carcinoma of the Breast Associated with Mixed Lobular and Ductal Carcinoma In Situ: A Case Report
- Apocrine Ductal Carcinoma In Situ of the Breast Presented Mass with Morphological Change on Follow-Up Ultrasound: A Report of Case
- Preoperative Breast Magnetic Resonance Imaging for the Assessment of the Size of Ductal Carcinoma In Situ
- The Role of Preoperative Magnetic Resonance Imaging for Detecting the Extent of Disease and Predicting the Prognosis of Ductal Carcinoma In Situ
