A rare goblet cell adenocarcinoma arising from Barrett’s esophagus: the first reported case in the esophagus
- Affiliations
-
- 1Department of Pathology, Kosin University College of Medicine, Busan, Korea
- 2Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea
- KMID: 2553475
- DOI: http://doi.org/10.4132/jptm.2023.12.26
Abstract
- Goblet cell adenocarcinoma (GCA) is a rare and distinctive amphicrine tumor comprised of goblet-like mucinous cells and neuroendocrine cells. It is believed to originate from pluripotent stem cells located at the base of crypts. GCA predominantly arises from the appendix, with a few reported cases in extra-appendiceal locations such as the colorectum, small intestine, and stomach. In this case report, we present a unique instance of a 64-year-old male who initially received a diagnosis of neuroendocrine carcinoma in the distal esophagus based on biopsy but, following resection, was subsequently re-diagnosed with GCA arising from Barrett’s esophagus.
Figure
-
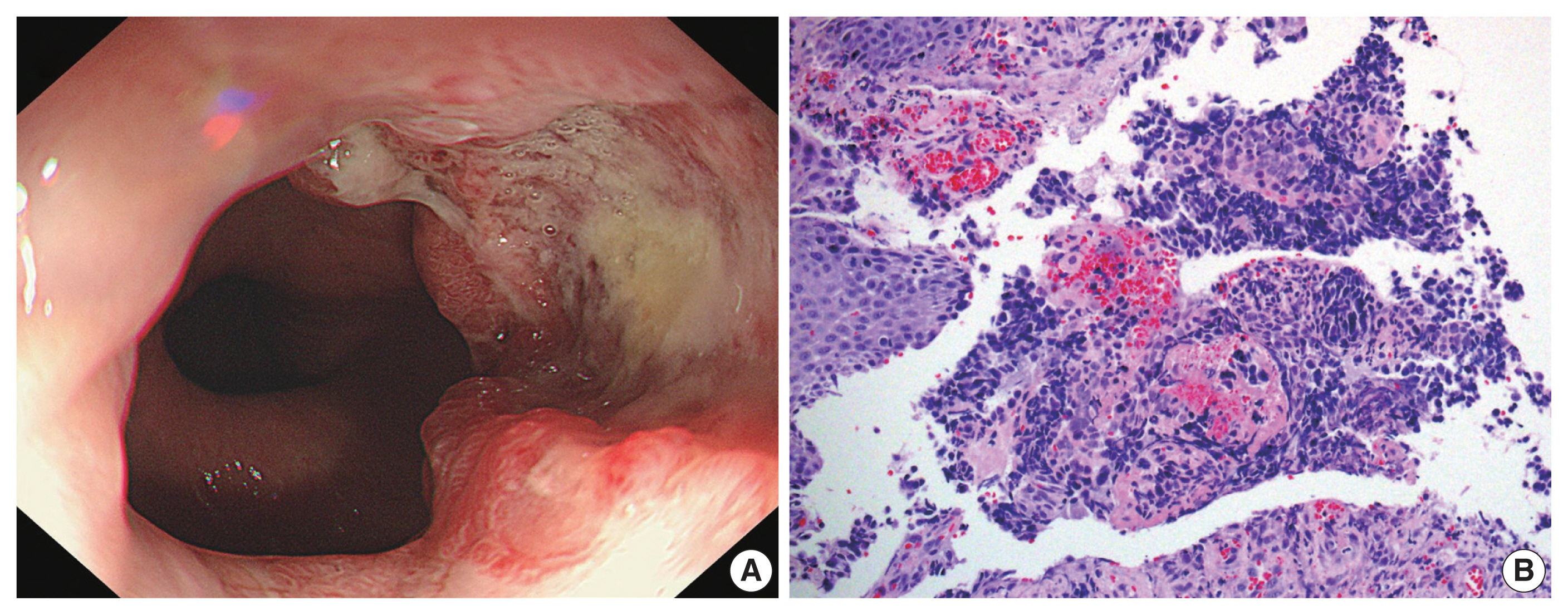
Fig. 1 (A) Gastroesophageal endoscopy revealed a mass with a central ulcer and irregular borders that almost completely encircled the esophageal lumen. (B) The biopsy showed sheets of tumor cells with hyperchromatic nuclei and minimal cytoplasm (right) along with normal esophageal squamous epithelium without dysplasia (left).

Fig. 2 (A) The gross examination of the resected tumor showed an ill-defined ulcerofungating firm mass in the distal esophagus, with the tip of the mass reaching the gastroesophageal junction. (B) Low magnification showed tumor cells penetrating the proper muscle layer and infiltrating the adventitia. (C) The gastroesophageal junction revealed esophageal squamous cells on the surface showing intestinal metaplasia (arrows), corresponding Barrett’s esophagus. At the base of the epithelium, a poorly differentiated single-file growth pattern of tumor cells was observed at the bottom with tumor glands with lumen observable at the top. (D) On high magnification in the low-grade tumor area, tumor cells exhibited a goblet cell morphology with intracytoplasmic mucin.

Fig. 3 (A) The tumor exhibited cribriform architecture and a single-file growth pattern at the lower and higher-grade regions, which contrasts with the more well-differentiated tumor components featuring glandular structures at the top. (B) Staining for synaptophysin highlights variable numbers of endocrine cells in immunohistochemical staining. (C) The Ki-67 labeling index was greater than 90%. (D) The tumor cells exhibited positive staining for luminal and intracytoplasmic mucin with alcian blue pH 2.5.
Reference
-
References
1. Zhang K, Meyerson C, Kassardjian A, Westbrook LM, Zheng W, Wang HL. Goblet cell carcinoid/carcinoma: an update. Adv Anat Pathol. 2019; 26:75–83.2. Gui X, Qin L, Gao ZH, Falck V, Harpaz N. Goblet cell carcinoids at extraappendiceal locations of gastrointestinal tract: an under-recognized diagnostic pitfall. J Surg Oncol. 2011; 103:790–5.3. Kang Y, Choi JW, Kim Y, Oh HE, Lee JH, Kim YS. Goblet cell carcinoid of the rectum in a patient with neurofibromatosis type 1. J Pathol Transl Med. 2016; 50:482–5.4. Lenti MV, Peri A, D’Ambrosio G, Gallo V, Di Sabatino A, Vanoli A. Primary appendiceal-type goblet cell adenocarcinoma of the ileum mimicking an inflammatory stricture in a woman with Crohn’s disease. Dig Liver Dis. 2021; 53:506–8.5. Murickan T, Onyemkpa C, Flynn C, Kavuturu S. Extra-appendiceal goblet cell carcinoid of the ascending colon. ACS Case Rev Surg. 2020; 2:66–70.6. Inoue Y, Horie H, Homma Y, et al. Goblet cell carcinoid of the rectum: a case report. Surg Case Rep. 2020; 6:174.7. Lewin K. Carcinoid tumors and the mixed (composite) glandular-endocrine cell carcinomas. Am J Surg Pathol. 1987; 11:Suppl 1. 71–86.8. Toumpanakis C, Standish RA, Baishnab E, Winslet MC, Caplin ME. Goblet cell carcinoid tumors (adenocarcinoid) of the appendix. Dis Colon Rectum. 2007; 50:315–22.9. Yozu M, Johncilla ME, Srivastava A, et al. Histologic and outcome study supports reclassifying appendiceal goblet cell carcinoids as goblet cell adenocarcinomas, and grading and staging similarly to colonic adenocarcinomas. Am J Surg Pathol. 2018; 42:898–910.10. Huang D, Ren F, Ni S, et al. Amphicrine carcinoma of the stomach and intestine: a clinicopathologic and pan-cancer transcriptome analysis of a distinct entity. Cancer Cell Int. 2019; 19:310.11. Roy P, Chetty R. Goblet cell carcinoid tumors of the appendix: an overview. World J Gastrointest Oncol. 2010; 2:251–8.12. Tang LH, Shia J, Soslow RA, et al. Pathologic classification and clinical behavior of the spectrum of goblet cell carcinoid tumors of the appendix. Am J Surg Pathol. 2008; 32:1429–43.13. Palmer K, Weerasuriya S, Chandrakumaran K, et al. Goblet cell adenocarcinoma of the appendix: a systematic review and incidence and survival of 1,225 cases from an English cancer registry. Front Oncol. 2022; 12:915028.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Esophageal Adenocarcinoma in Barrett's Esophagus: A case report
- A Case of Esophageal Adenocarcinoma Arising from a Short Segment of Barrett's Esophagus
- Esophagus, Stomach & Intestine; Adenocarcinoma Arising from Barrett's Esophagus: A case report
- Treatment of Barrett's Esophagus
- Epidemiology of Barrett's Esophagus
