An anatomical investigation of the suboccipitaland inferior suboccipital triangles
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine, University of Pretoria, Pretoria, South Africa
- KMID: 2546463
- DOI: http://doi.org/10.5115/acb.23.015
Abstract
- The suboccipital triangle (ST) is a clinically relevant landmark in the posterior aspect of the neck and is used to locate and mobilize the horizontal segment of the third part of the vertebral artery before it enters the cranium. Unfortunately, this space is not always a viable option for vertebral artery exposition, and consequently a novel triangle, the inferior suboccipital triangle (IST) has been defined. This alternative triangle will allow surgeons to locate the artery more proximally, where its course is more predictable. The purpose of this study was to better define the anatomy of both triangles by measuring their borders and calculating their areas. Ethical clearance was obtained from the University of Pretoria (reference number: 222/2021) and both triangles were subsequently dissected out on both the left and right sides of 33 formalin-fixed human adult cadavers. The borders of each triangle were measured using a digital calliper and the areas were calculated using Herons Formula. The average area of the ST is 969.82±153.15 mm 2 , while the average area of the IST is 307.48±41.31 mm 2 . No statistically significant differences in the findings were observed between the sides of the body, ancestry, or sex of the cadavers. Measurement and analysis of these triangles provided important anatomical information and speak to their clinical relevance as surgical landmarks with which to locate the vertebral artery. Of particular importance here is the IST, which allows for mobilisation of this artery more proximally, should the ST be occluded.
Keyword
Figure
-

Fig. 1 Specimen image illustrating the borders of the ST (blue) and IST (yellow) triangle, indicating that the vertebral artery runs through both triangles. ST, suboccipital triangle; IST, inferior suboccipital triangle.
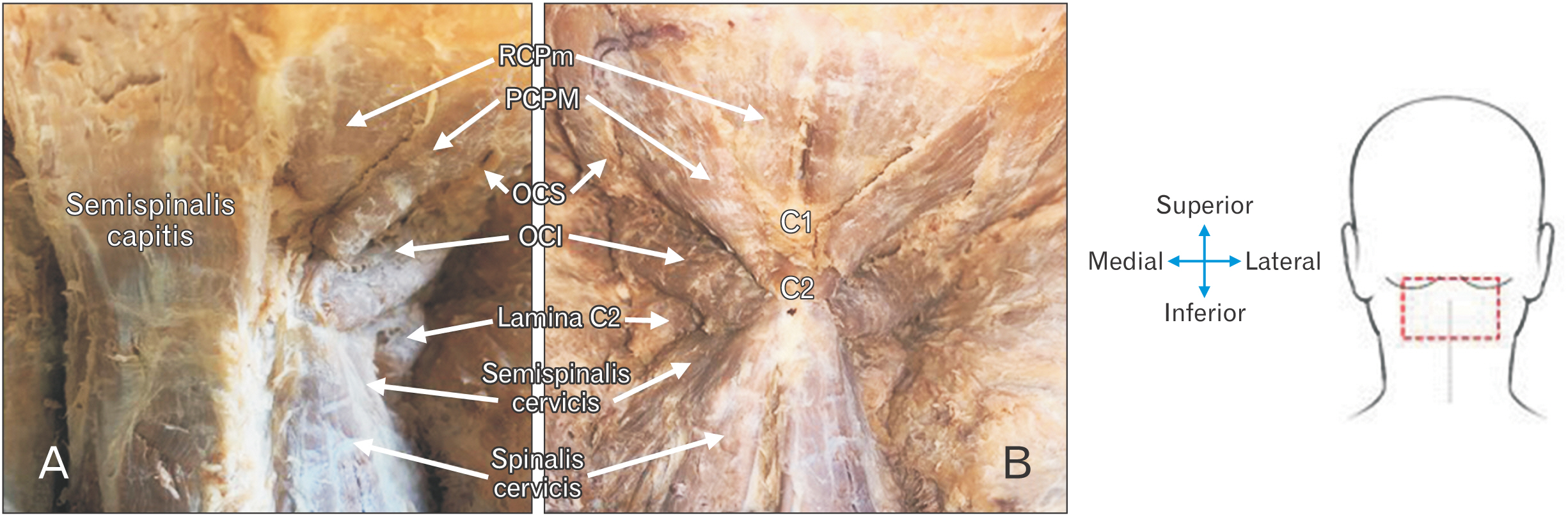
Fig. 2 (A) Image of exposed right suboccipital region with the right ST and IST and associated muscles visible, while the left semispinalis is still intact, covering the left ST and IST. (B) Image of trapezius, splenius capitis, semispinalis capitis muscles reflected to expose both the left and right suboccipital regions. ST, suboccipital triangle; IST, inferior suboccipital triangle; RCPm, rectus capitis posterior minor; RCPM, rectus capitis posterior major; OCS, obliquus capitis superior; OCI, obliquus capitis inferior.
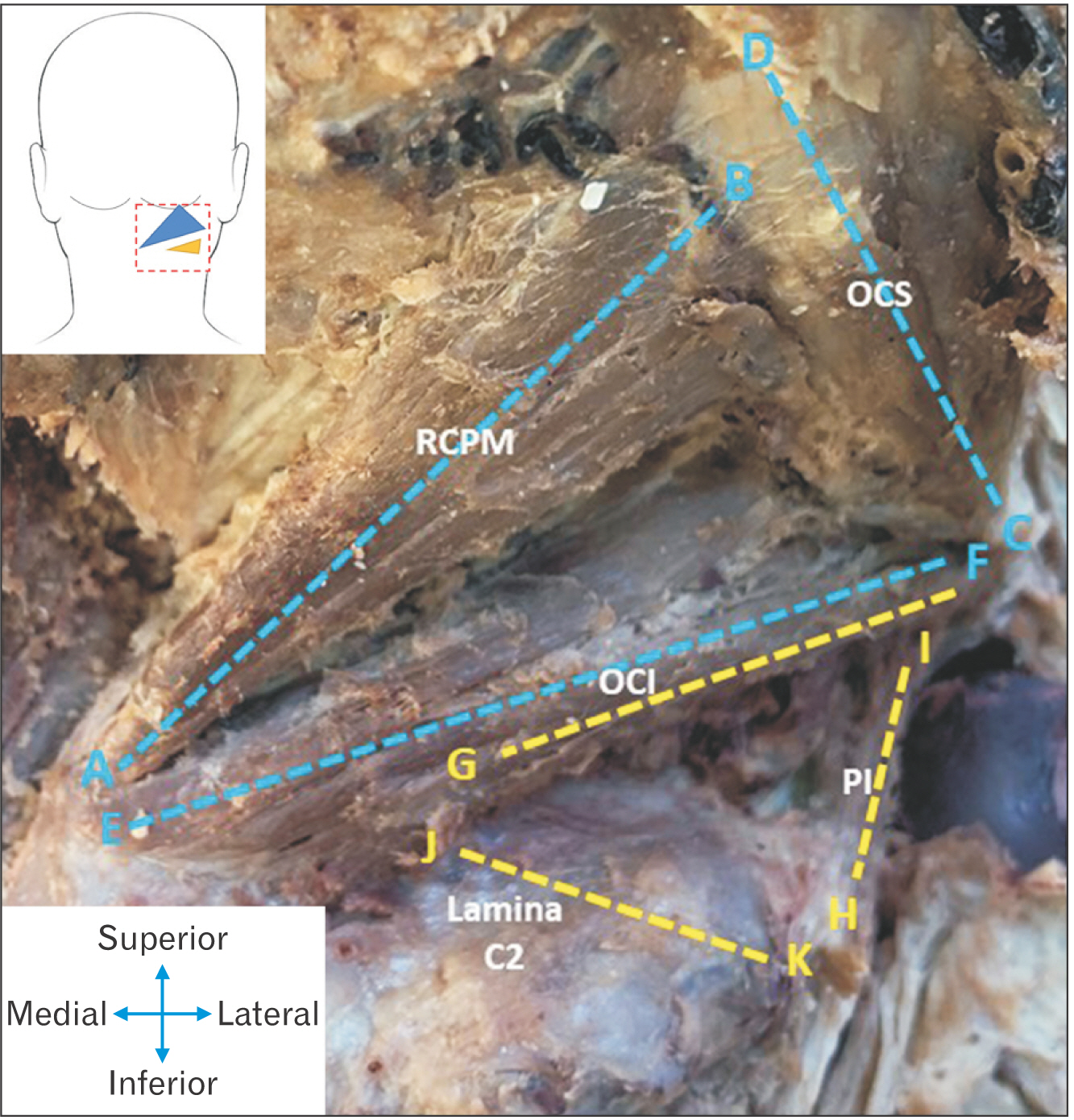
Fig. 3 Image indicating the relevant measurements taken for both the ST (blue measurements) and the IST (yellow measurements). ST, suboccipital triangle; IST, inferior suboccipital triangle; RCPM, rectus capitis posterior major; OCS, obliquus capitis superior; OCI, obliquus capitis inferior; PI, posterior intertransversarii.

Fig. 4 Average lengths (mm) obtained of all the borders of the triangles. Comparing these measurements for the black- and white ancestry groups (A), females, males (B) as well as left- and right sides (C). Letters in brackets refer to the reference points inserted, and distance measured between the points.
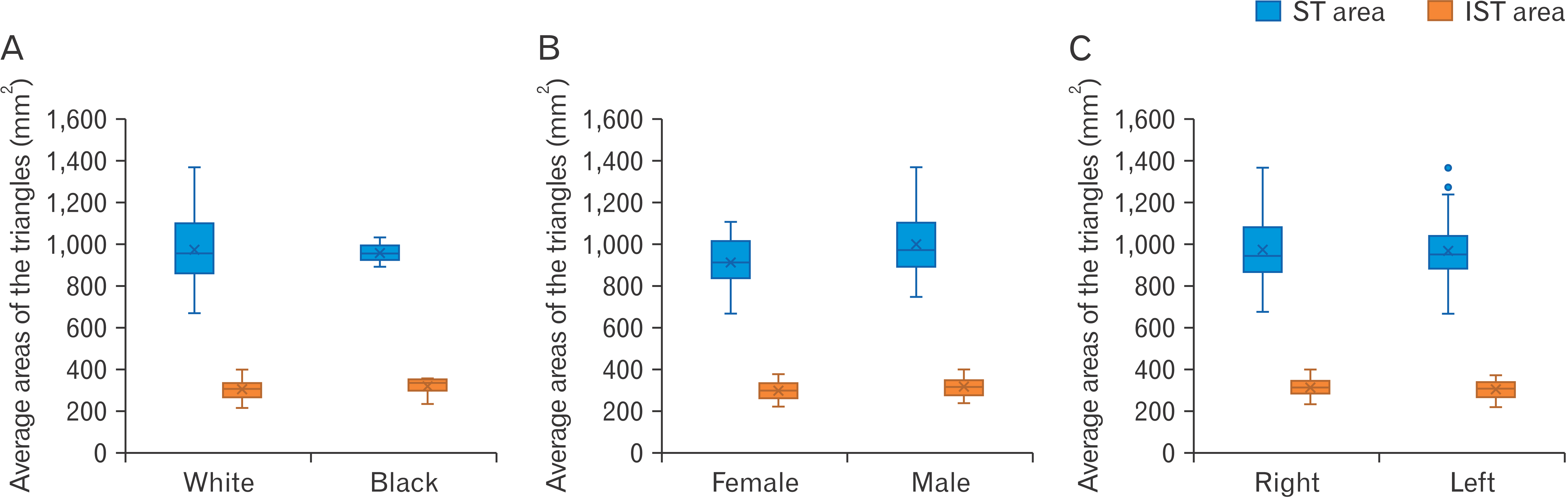
Fig. 5 Average areas (mm2) obtained for the suboccipital triangle (ST) and the inferior suboccipital triangle (IST). Comparing these areas for the black- and white ancestry groups (A), females, males (B) as well as left- and right sides (C).
Reference
-
References
1. Standring S. 2016. Gray's anatomy: the anatomical basis of clinical practice. 41st ed. Elsevier;p. 457–8. p. 744–5.2. Kikuta S, Iwanaga J, Kusukawa J, Tubbs RS. 2019; Triangles of the neck: a review with clinical/surgical applications. Anat Cell Biol. 52:120–7. DOI: 10.5115/acb.2019.52.2.120. PMID: 31338227. PMCID: PMC6624334.
Article3. Yamauchi M, Yamamoto M, Kitamura K, Morita S, Nagakura R, Matsunaga S, Abe S. 2017; Morphological classification and comparison of suboccipital muscle fiber characteristics. Anat Cell Biol. 50:247–54. DOI: 10.5115/acb.2017.50.4.247. PMID: 29354295. PMCID: PMC5768560.
Article4. George T, Tadi P. 2022. Anatomy, head and neck, suboccipital muscles [Internet]. StatPearls;Available from: https://www.ncbi.nlm.nih.gov/books/NBK567762/. cited 2022 Nov 25.5. Sriamornrattanakul K, Akharathammachote N, Chonhenchob A, Mongkolratnan A, Niljianskul N, Phoominaonin IS, Ariyaprakai C, Wongsuriyanan S. 2022; Course of the V3 segment of the vertebral artery relative to the suboccipital triangle as an anatomical marker for a safe far lateral approach: a retrospective clinical study. Surg Neurol Int. 13:304. DOI: 10.25259/SNI_346_2022. PMID: 35928311. PMCID: PMC9345113.
Article6. Arnautović KI, Al-Mefty O. 2002; The microsurgical anatomy of the suboccipital vertebral artery and its surrounding structures. Oper Tech Neurosurg. 5:1–10. DOI: 10.1053/otns.2002.31255.
Article7. Tjahjadi M, Rezai Jahromi B, Serrone J, Nurminen V, Choque-Velasquez J, Kivisaari R, Lehto H, Niemelä M, Hernesniemi J. 2017; Simple lateral suboccipital approach and modification for vertebral artery aneurysms: a study of 52 cases over 10 years. World Neurosurg. 108:336–46. DOI: 10.1016/j.wneu.2017.09.014. PMID: 28899830.
Article8. Fisahn C, Burgess B, Iwanaga J, Alonso F, Chapman JR, Oskouian RJ, Tubbs RS. 2017; A previously unreported arterial variant of the suboccipital region based on cadaveric dissection. J Neurol Surg Rep. 78:e40–2. DOI: 10.1055/s-0037-1600136. PMID: 28299248. PMCID: PMC5350074. PMID: 5b510616e1e44ec39f00fbd374421a9f.
Article9. La Rocca G, Altieri R, Ricciardi L, Olivi A, Della Pepa GM. 2017; Anatomical study of occipital triangles: the 'inferior' suboccipital triangle, a useful vertebral artery landmark for safe postero-lateral skull base surgery. Acta Neurochir (Wien). 159:1887–91. DOI: 10.1007/s00701-017-3300-3. PMID: 28828558.
Article10. Molinari RW, Chimenti PC, Molinari R Jr, Gruhn W. 2015; Vertebral artery injury during routine posterior cervical exposure: case reports and review of literature. Global Spine J. 5:528–32. DOI: 10.1055/s-0035-1566225. PMID: 26682106. PMCID: PMC4671909.
Article11. George B, Blanquet A, Alves O. 2002; The V3 segment of the vertebral artery: surgery around the craniocervical junction. Oper Tech Neurosurg. 5:50–74. DOI: 10.1053/otns.2002.000.
Article12. Khanfour AA, El Sekily NM. 2015; Relation of the vertebral artery segment from C1 to C2 vertebrae: an anatomical study. Alex J Med. 51:143–51. DOI: 10.1016/j.ajme.2014.05.007.
Article13. Balik V, Takizawa K. 2019; Safe and bloodless exposure of the third segment of the vertebral artery: a step-by-step overview based on over 50 personal cases. Neurosurg Rev. 42:991–7. DOI: 10.1007/s10143-019-01158-5. PMID: 31410682.
Article14. Detton AJ. 2016. Grant's dissector. 16th ed. Wolters Kluwer;p. 16–7. DOI: 10.1007/springerreference_12767.15. Lowry HV. 1964; Heron's formula. Math Gaz. 48:312–3. DOI: 10.2307/3613028.16. Kalmanson OA, Khayatzadeh S, Germanwala A, Scott-Young M, Havey RM, Voronov LI, Patwardhan AG. 2019; Anatomic considerations in headaches associated with cervical sagittal imbalance: a cadaveric biomechanical study. J Clin Neurosci. 65:140–4. DOI: 10.1016/j.jocn.2019.02.003. PMID: 30876933.
Article17. Muralimohan S, Pande A, Vasudevan MC, Ramamurthi R. 2009; Suboccipital segment of the vertebral artery: a cadaveric study. Neurol India. 57:447–52. DOI: 10.4103/0028-3886.55610. PMID: 19770546.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Triangles of the neck: a review with clinical/surgical applications
- A Study on the Anatomical Position of the Inferior Oblique Muscle Insertion in Primary Inferior Oblique Overaction
- Surgical Treatment by the Far Lateral Inferial Suboccipital Approach for the Distal Vertebral Artery Aneurysm
- A Case of Bilateral Bridges of a Korean Atlas
- Clinical Experiences of Trigeminal Rhizotomy using Suboccipital Approach
