A rare case of sacral epidural arteriovenous fistula with concomitant occult multiple lumbar epidural arteriovenous fistulas
- Affiliations
-
- 1Department of Neurosurgery, Saiseikai Utsunomiya Hospital, Utsunomiya, Tochigi, Japan
- 2Department of Radiology, Ashikaga Red Cross Hospital, Ashikaga, Tochigi, Japan
- 3Department of Radiology, Saiseikai Utsunomiya Hospital, Utsunomiya, Tochigi, Japan
- KMID: 2546170
- DOI: http://doi.org/10.7461/jcen.2022.E2022.07.002
Abstract
- We describe a rare case of sacral epidural arteriovenous fistulas (edAVFs) with atypical clinical course of treatment. A 78-year-old man with a history of spinal surgery presented progressive gait disturbance and urinary incontinence. Spinal angiography demonstrated a sacral spinal AVF fed by bilateral lateral sacral arteries, draining to the venous pouch with subdural drainage. The first treatment by direct interruption of a subdural drainer was incompletely finished. Postoperative reassessment by 3D imaging analysis led to the diagnosis of sacral edAVF and 3D understanding of its angioarchitecture. The second treatment by transarterial embolization (TAE) resulted in complete occlusion of a sacral edAVF. However, spinal venous congestion didn’t improve, because the recruitment of occult edAVFs at the multiple lumbar levels and complex-shaped sacral ventral epidural venous plexus (VEP) were involved in the remnant of prior subdural drainage. The third treatment was performed by TAE for three occult edAVFs and the VEP compartment connecting between a patent edAVF and subdural drainage, which resulted in complete disappearance of spinal cord edema. Endovascular embolization of VEP compartment connecting to subdural drainage in addition to fistulous occlusion may be one of the treatment options for several edAVFs at the multiple spinal levels.
Keyword
Figure
-
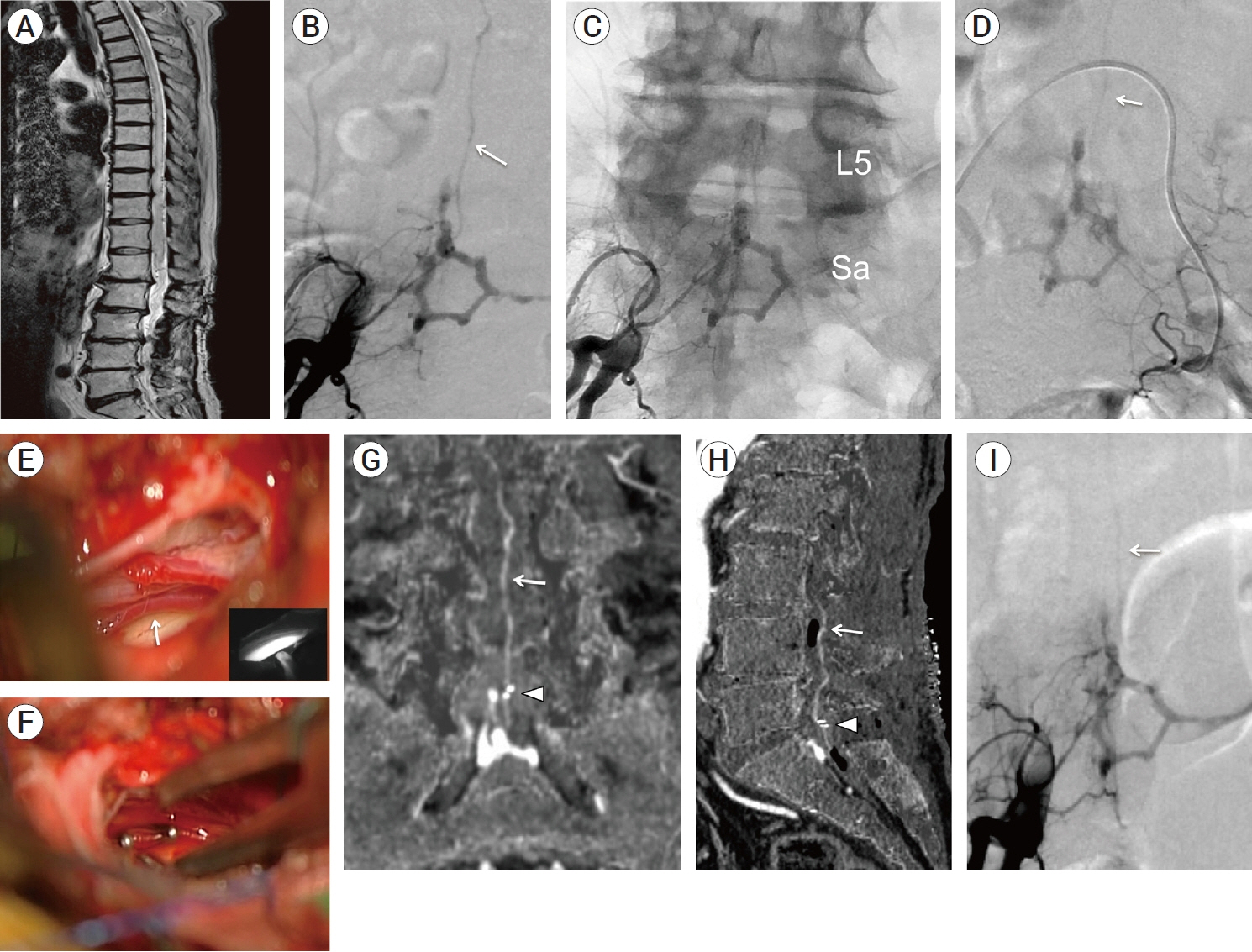
Fig. 1. (A) T2-weighted sagittal image of spine MRI, showing spinal cord swelling and vascular flow voids. (B-D) Preoperative angiography (anterior-posterior view) of right and left internal iliac arteries (B: subtracted digital image, C: non-subtracted digital image, D: subtracted digital image). Bilateral lateral sacral arteries collected to the shunt points on the upper compartment of hexagonal- shaped venous pouch and a subdural drainer (white arrow) arising from the venous pouch ran upward. (E-F) Intraoperative photograph during intradural exploration. (E) A radicular vein (white arrow) intermingled with the nerve roots was suspicious of a target subdural drainer. Indocyanine green videoangiograpy (presented in the small boxed area) demonstrated that the radicular vein was arterialized. (F) The arterialized radicular vein was clipped by two Weck® ligating clips (Teleflex, Research Triangle Park, USA). (G-I) Postoperative digital-subtraction CTA images and digital-subtraction angiogram. (G) Coronal MIP image and (H) sagittal MIP image produced from digital-subtraction CTA data, indicating the remnant of a subdural drainer (white arrow) despite the closure by two clips (white arrowhead). (I) Postoperative digital-subtraction angiogram (anterior-posterior view) of a right internal iliac artery showed that a residual subdural drainer (white arrow), while its visualization seemed to reduce due to the clip interruption. L5, fifth lumbar vertebrae; Sa, sacral vertebrae; MIP, maximum intensity projection
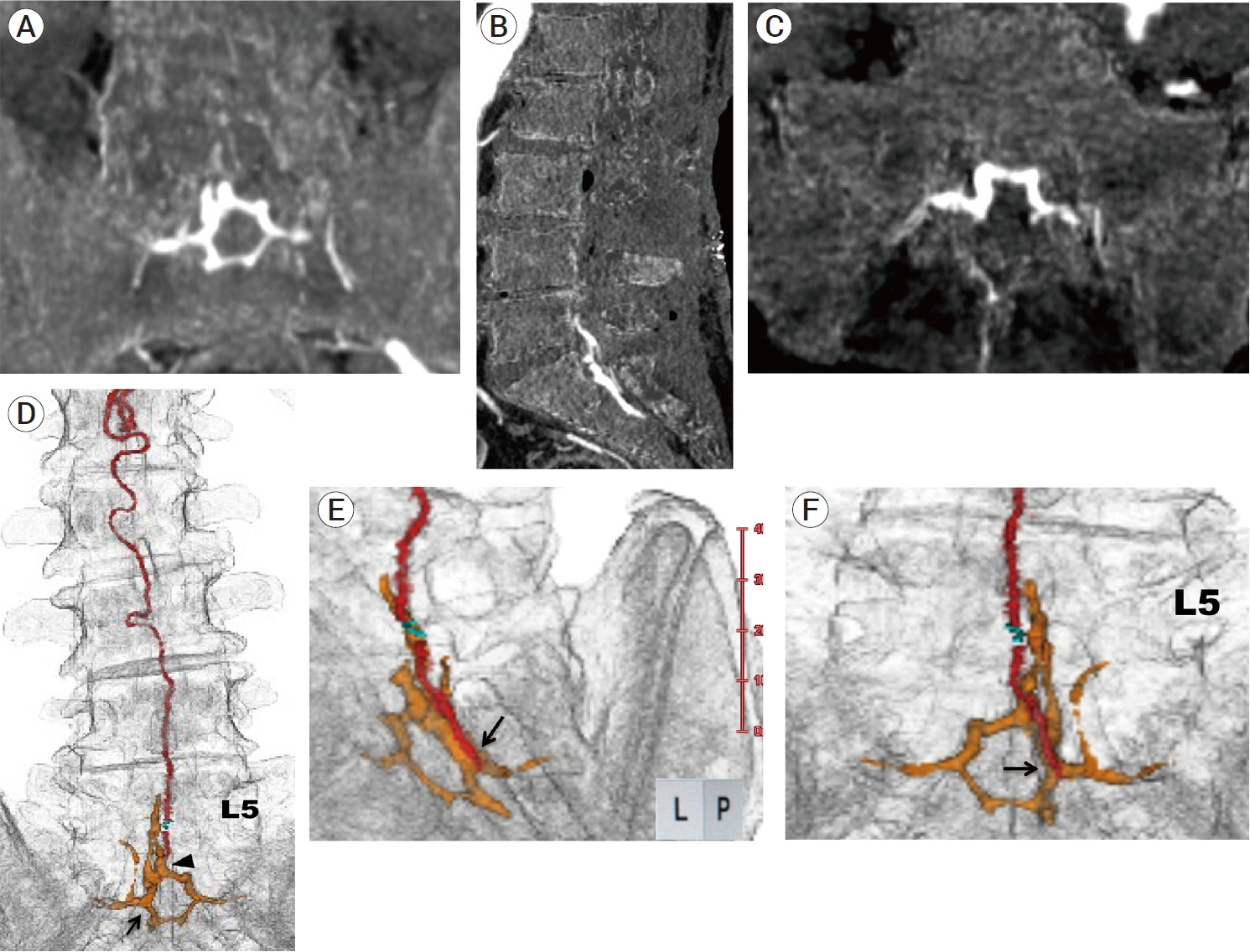
Fig. 2. (A-C) Postoperative MIP images produced from digital-subtraction CTA data (A: coronal section, B: sagittal section, C: axial section), showing that a hexagonal venous pouch with subdural drainage was found to be the enlarged VEP at the L5-S1 spinal levels. (D-F) Postoperative 3D multifusion images produced from CTA data (D: anterior-posterior view, E: magnified left posterolateral view, F: magnified posterior-anterior view), showing the positional relationship among VEP (orange color), a subdural drainer (red color), Weck® ligating clips (Teleflex, Research Triangle Park, USA) (green color) and a lumbosacral vertebrae. 3D multifusion images also revealed that a subdural drainer arose from the lower compartment (black arrow) of sacral VEP, indicating that the origin of a subdural drainer was very distant from the shunt points (black arrowhead) on the upper compartment of sacral VEP. MIP, maximum intensity projection; VEP, ventral epidural venous plexus; L5, fifth lumbar vertebrae
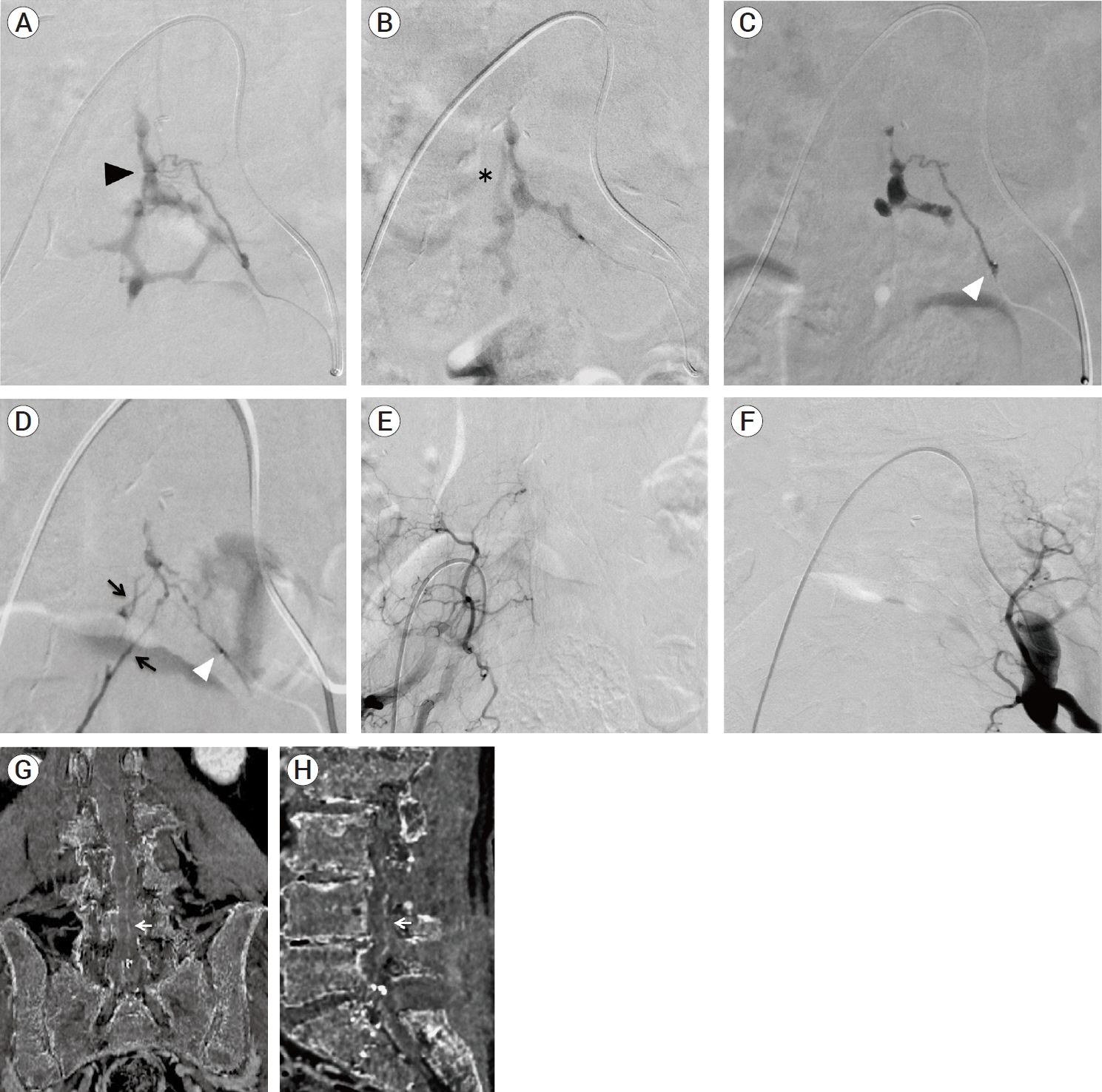
Fig. 3. (A-C) Superselective angiograms of a feeder branching from a left lateral sacral artery during the first session of endovascular treatment. (A) In the arterial early phase, a hexagonal-shaped VEP and a shunt point (black arrowhead) were clearly observed. (B) In the arterial late phase, a two-lane route (asterisk) of venous drainage in the upper part of a hexagonal-shaped sacral VEP appeared in a slightly delayed fashion, indicating that there was a two-lane venous connection between a lumbar and a sacral VEP. (C) The first injection of 11% warming NBCA from a feeder branching from a left lateral sacral artery resulted in the glue penetration to the upper compartment of sacral VEP. White arrowhead indicates the tip of microcatheter. (D) The second injection of 11% warming NBCA from another feeder branching from a left lateral sacral artery resulted in a slight glue penetration through another shunt point to the remaining upper compartment of sacral VEP, followed by the glue penetration to contralateral feeders (black arrow) via the retrocorporeal anastomosis. (E, F) Angiograms of bilateral internal iliac arteries (E: right side, F: left side) showed the complete occlusion of the sacral edAVF. (G, H) MIP images produced from digital-subtraction CTA data (G: coronal section, H: sagittal section) after the first session of endovascular treatment, showing that a subdural drainer became poorly visualized but still remaining (white arrow). VEP, ventral epidural venous plexus; NBCA, n-butyl-2-cyanoacrylate; MIP, Maximum intensity projection; edAVF, epidural arteriovenous fistula
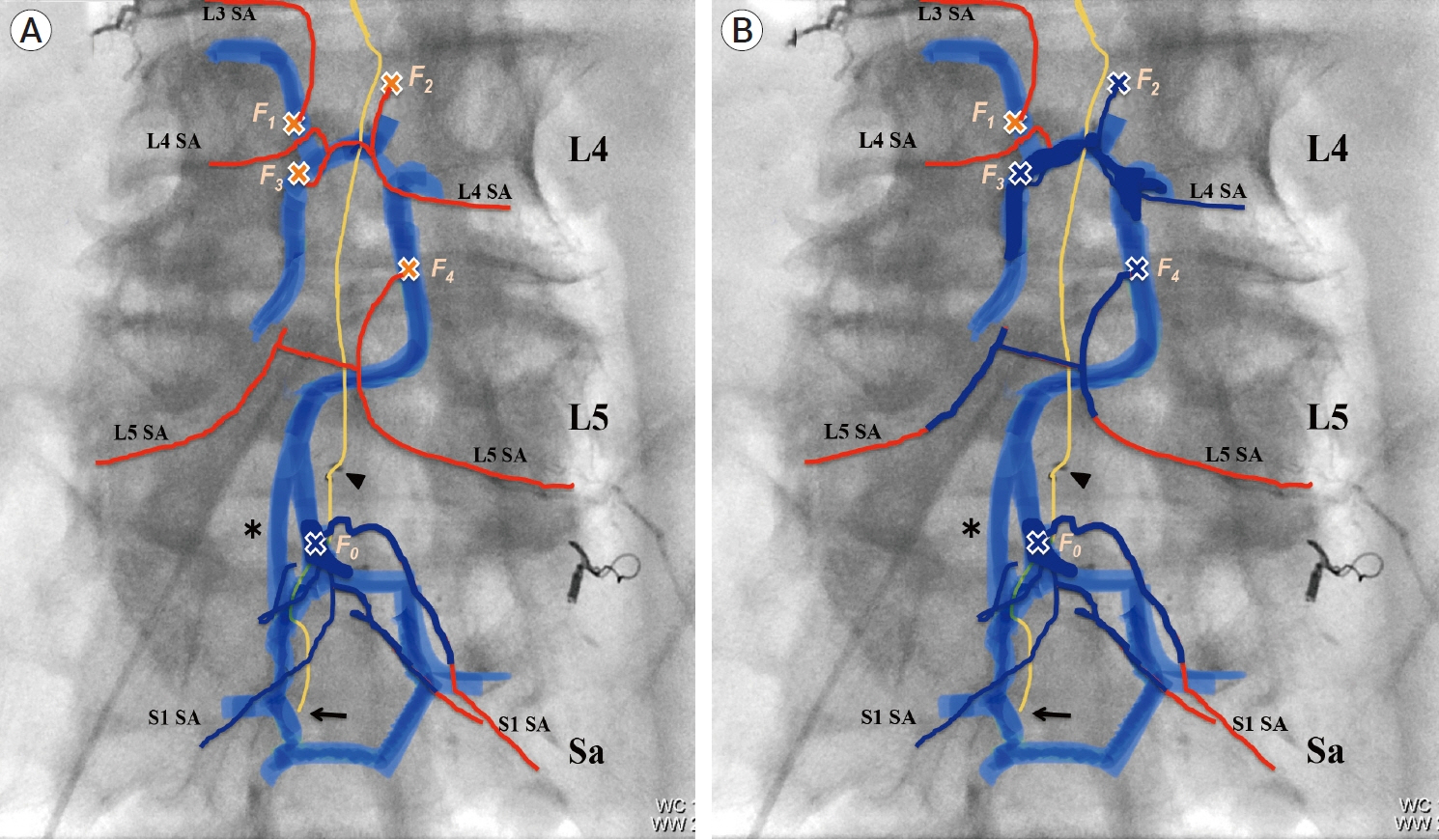
Fig. 4. Schematic illustration of whole vascular architecture related to multiple spinal edAVF. (red color line: feeders, blue color band line: longitudinal VEP, yellow color line: a subdural drainer, black arrowhead: Weck® ligating clips (Teleflex, Research Triangle Park, USA), orange cross mark: fistula point). Every fistula is numbered from 0-4 in the cream color. Asterisk indicates a two-lane venous route between lumbar and sacral VEP. Black arrow indicates the origin of a subdural drainer. (A) After the first session of endovascular treatment. A part of sacral VEP, F4 fistula, and feeders filling with NBCA casts were represented by navy blue color. The recruitment of occult four fistulas (F1- F4) fed by L3-L5 segmental arteries was newly observed. Shunt blood flow from new four fistulas drained into the lumbar VEP with ladder- shape. Shunt blood flow from lumbar edAVFs ran downward to the sacral VEP. (B) After the second session of endovascular treatment. The compartment of longitudinal VEP, fistulas, and feeders filling with NBCA casts were represented by navy blue color. Eventually, four fistulas (F0 and F2-F4) were completely occluded by two sessions of endovascular treatment. Although F1 fistula was patent due to feeder occlusion, shunt blood flow from F1 fistula was blocked by NBCA casts. The epidural venous connection between all fistulas (F0-F4) and a subdural drainer was interrupted by TAE, suggesting that an arterialized subdural drainer became normalized or occluded theoretically. edAVF, epidural arteriovenous fistula; VEP, ventral epidural venous plexus; NBCA, n-butyl-2-cyanoacrylate; TAE, transarterial embolizaion; SA, segmental artery
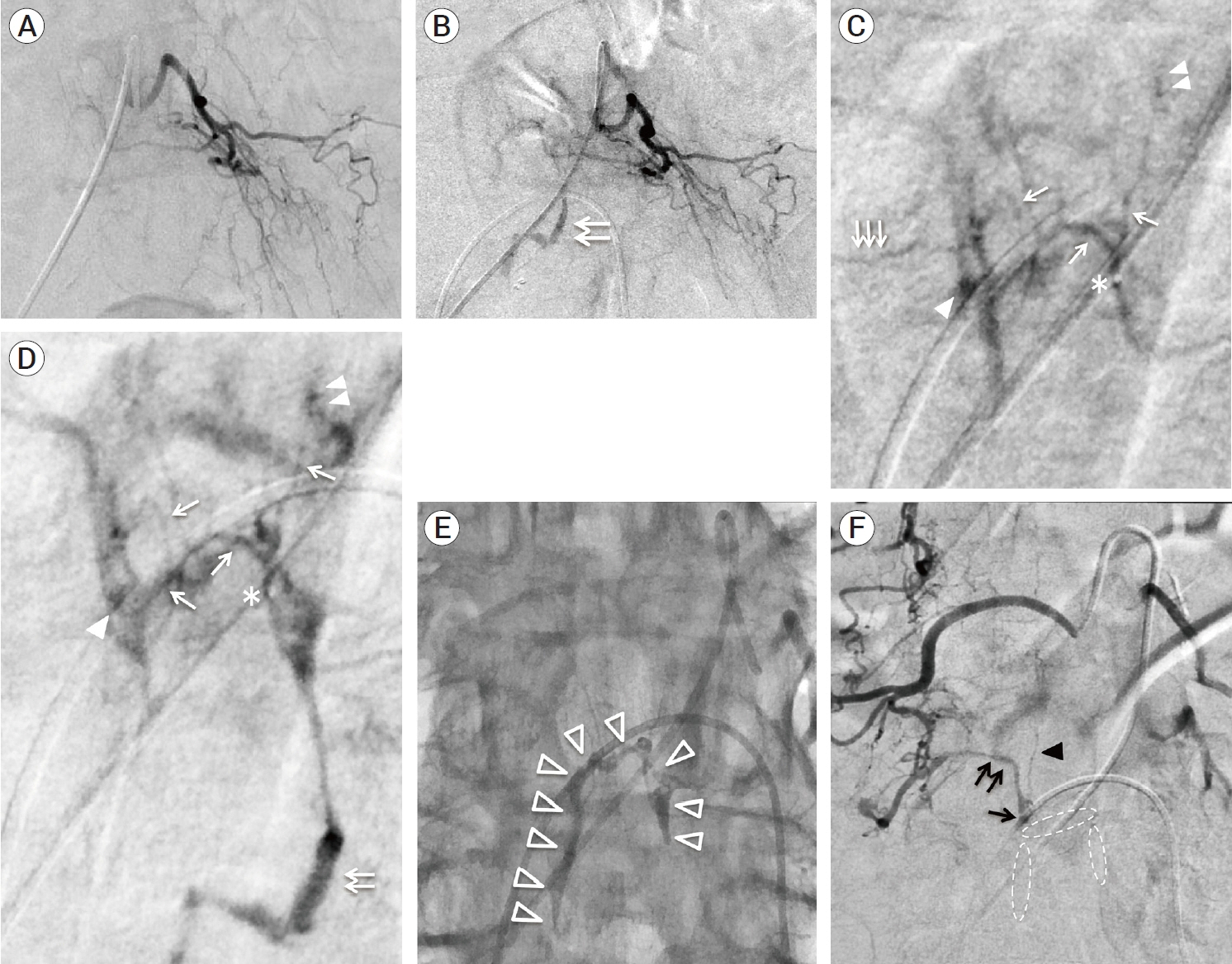
Fig. 5. Representative angiograms from (A-E) a left L4 segmental artery and (F) a right L3 segmental artery. (A-B) Angiograms of a left L4 segmental angiography (A: before TAE, B: after the first session of TAE). After the first session of TAE, the shunted lumbar VEP (white double arrows) newly appeared. (C-D) Superselective angiograms from the distal portion of a left L4 segmental artery (C: arterial early phase, D: arterial late phase). The asterisk indicates the tip of microcatheter. The white single arrows indicate feeders branching from a left L4 segmental artery. The white triple arrows indicate a feeder branching from a right L4 segmental artery. These angiograms showed the early filling of ladder shaped VEP via F2 (white double arrowheads) and F3 fistulas (white single arrowhead), followed by descending epidural venous drainage (white double arrows) toward sacral VEP. (E) Fluoroscopic image after TAE, showing NBCA casts (white open arrowheads) filling in the partial VEP including F2 and F3 fistulas. (F) Angiogram of right L3 segmental angiography, showing the prior NBCA casts (white dotted ellipse) blocked the shunt blood flow from F1 fistula (black single arrow) toward ladder shaped VEP. The shunt blood flow from F1 fistula connected to only the paravertebral drainage (black double arrow). Black arrowhead indicates a feeder branching from right L3 segmental artery. TAE, transarterial embolization; VEP, ventral epidural venous plexus; NBCA, n-butyl-2-cyanoacrylate
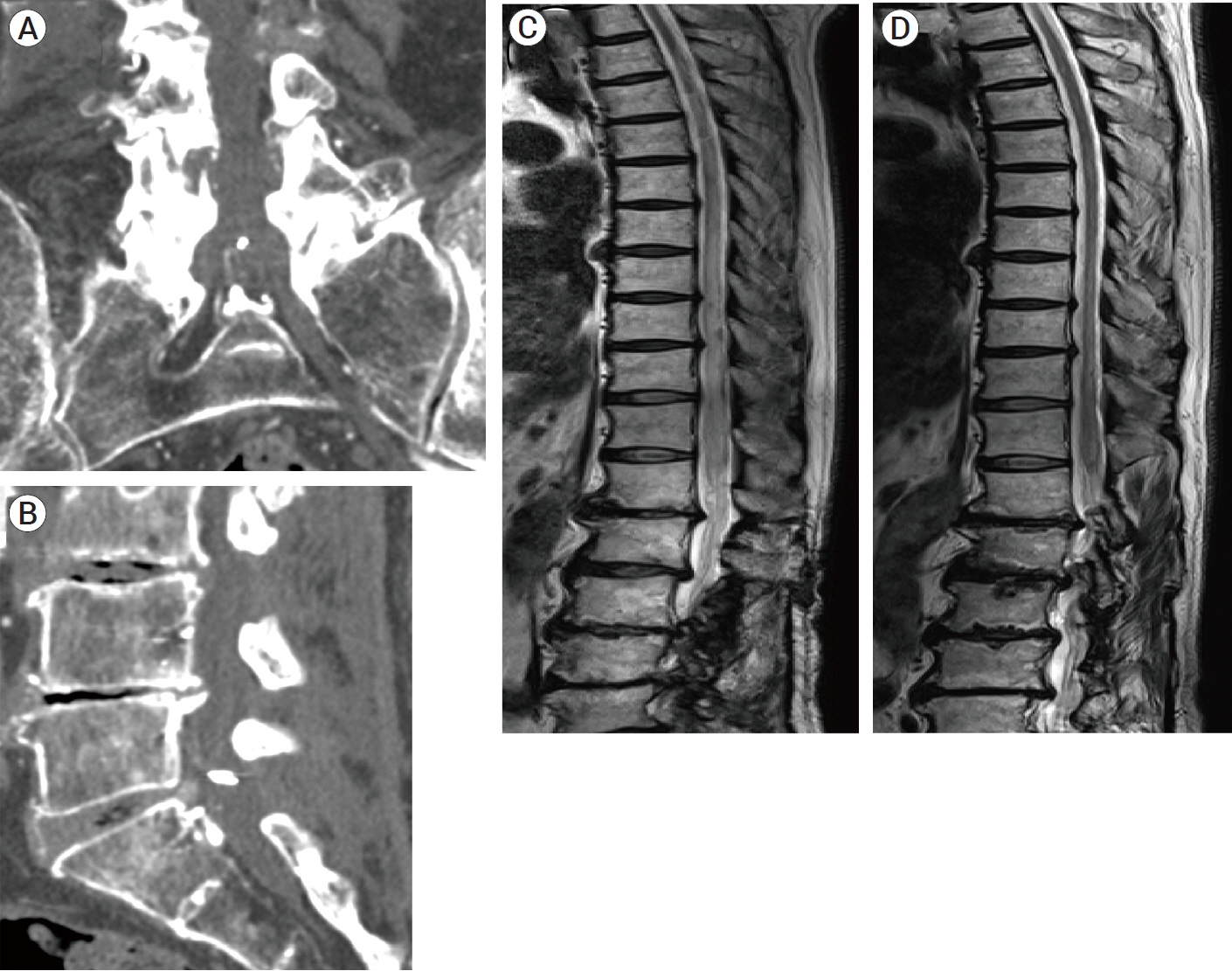
Fig. 6. Postoperative follow-up CTA and MRI after the third treatment. (A, B) MIP images produced from CTA data (A: coronal section, B: sagittal section), showing the disappearance of a subdural drainer. (C, D) T2-weighted sagittal images of spine MRI after the third treatment (C: after three months, D: after ten months), showing that spinal cord edema gradually decreased and eventually disappeared without any vessel flow voids. MIP, maximum intensity projection
Reference
-
1. Alvarado AM, Haussen DC, Ebersole K, Nogueira RG, Abraham MG. Embolization of sacral dural arteriovenous fistulas: a case series and literature review. Interv Neurol. 2017; Mar. 6(1-2):73–81.2. Burkhardt J, Safaee MM, Clark AJ, Lawton MT. Sacral epidural arteriovenous fistulas: imitators of spinal dural arteriovenous fistulas with different pathologic anatomy: report of three cases and review of the literature. Acta Neurochir. 2017; Jun. 159(6):1087–92.3. Clarke MJ, Patrick TA, White JB, Cloft HJ, Krauss WE, Lindell EP, et al. Spinal extradural arteriovenous malformations with parenchymal drainage: venous drainage variability and implications in clinical manifestations. Neurosurg Focus. 2009; Jan. 26(1):e5.4. Geibprasert S, Pereira V, Krings T, Jiarakongmun P, Toulgoat F, Pongpech S, et al. Dural arteriovenous shunts: a new classification of craniospinal epidural venous anatomical bases and clinical correlations. Stroke. 2008; Oct. 39(10):2783–94.5. Groen RJ, Groenewegen HJ, van Alphen HA, Hoogland PV. Morphology of the human internal vertebral venous plexus: a cadaver study after intravenous araldite CY 221 injection. Anat Rec. 1997; Oct. 249(2):285–94.6. Hiramatsu M, Sugiu K, Yasuhara T, Hishikawa T, Nishihiro S, Kidani N, et al. Comparison between spinal dural arteriovenous fistula and spinal epidural arteriovenous fistula. Journal of Neuroendovascular Therapy. 2019; Mar. 13(3):114–9.7. Kiyosue H, Ide S, Uchida S, Kubo T. Dural arteriovenous fistulas: interpretation from the view point of vascular anatomy. No Kekkannai Chiryo. 2020; Jan. 5(1):6–18.8. Kiyosue H, Matsumaru Y, Niimi Y, Takai K, Ishigro T, Hiramatsu M, et al. Angiographic and clinical characteristics of thoracolumbar spinal epidural and dural arteriovenous fistulas. Stroke. 2017; Dec. 48(12):3215–22.9. Krings T, Geibprasert S. Spinal dural arteriovenous fistulas. AJNR Am J Neuroradiol. 2009; Apr. 30(4):639–48.10. Lasjaunias P, Berenstein A, ter Brugge KG. Spinal and Spinal Cord Arteries and Veins. Clinical Vascular Anatomy and Variations. Volume 1, 2nd edition. Berlin, Heidelberg: Springer;2001. p. 73–160.11. Lenck S, Nicholson P, Tymianski R, Hilditch C, Nouet A, Patel K, et al. Spinal and paraspinal arteriovenous lesions. Stroke. 2019; Aug. 50(8):2259–69.12. Patsalides A, Knopman J, Santillan A, Tsiouris AJ, Riina H, Gobin YP. Endovascular treatment of spinal arteriovenous lesions: beyond the dural fistula. AJNR Am J Neuroradiol. 2011; May. 32(5):798–808.13. Ren Y, Liu H, Chen T, You C, Li J. Successful management of sacral dural arteriovenous fistulas: a case series and literature review. World Neurosurg. 2019; Jun. 126:164–70.14. Sasamori T, Hida K, Asano T, Aoyama T, Yamauchi T, Iwasaki M, et al. Sacral dural arteriovenous fistula. Spinal Surgery. 2011; Apr. 25(1):81–3.15. Tadie M, Hemet J, Aaron C, Bianco C, Creissard P, Huard P. Le dispositif protecteur anti-reflux des veines de la moelle. Neurochirurgie. 1979; 25:28–30.16. Takahashi K, Matsumoto Y, Nagata Y, Hashikawa T, Sakai H, Furuta K, et al. The shunt point of the sacral dural arteriovenous fistula: a case report and literature review. World Neurosurg. 2020; Nov. 143:518–26.17. Takai K, Endo T, Yasuhara T, Seki T, Watanabe K, Tanaka Y, et al. Microsurgical versus endovascular treatment of spinal epidural arteriovenous fistulas with intradural venous drainage: a multicenter study of 81 patients. J Neurosurg Spine. 2020; Apr. 24:1–11.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Spinal Dural and Epidural Arteriovenous Fistula as Complication of Lumbar Surgery
- Arteriovenous Fistula follwing Lumbar Discectomy
- Spinal Epidural Arteriovenous Fistula Presented with Subdural Hematoma: a Case of Transarterial Embolization Using NBCA
- Acute Paraplegia After Lumbar Steroid Injection in Patients With Spinal Dural Arteriovenous Fistulas: Case Reports
- Congenital Renal Arteriovenous Fistula
