Evaluation of a new method, “non-injection resection using bipolar soft coagulation mode (NIRBS)”, for colonic adenomatous lesions
- Affiliations
-
- 1Department of Gastroenterology, Japan Community Healthcare Organization Hoshigaoka Medical Center, Osaka, Japan
- 2Third Department of Internal Medicine, Division of Gastroenterology and Hepatology, Kansai Medical University Hirakata Hospital, Osaka, Japan
- 3Department of Hygiene and Public Health, Kansai Medical University Hirakata Hospital, Osaka, Japan
- KMID: 2546141
- DOI: http://doi.org/10.5946/ce.2022.200
Abstract
- Background/Aims
Endoscopic resection of all colorectal adenomatous lesions with a low complication rate, simplicity, and negative residuals is challenging. Hence, we developed a new method called “non-injection resection using bipolar soft coagulation mode (NIRBS)” method, adapted for colorectal lesions. In addition, we evaluated the effectiveness of this method.
Methods
We performed NIRBS throughout a 12-month period for all colorectal lesions which snare resection was acceptable without cancerous lesions infiltrating deeper than the submucosal layer.
Results
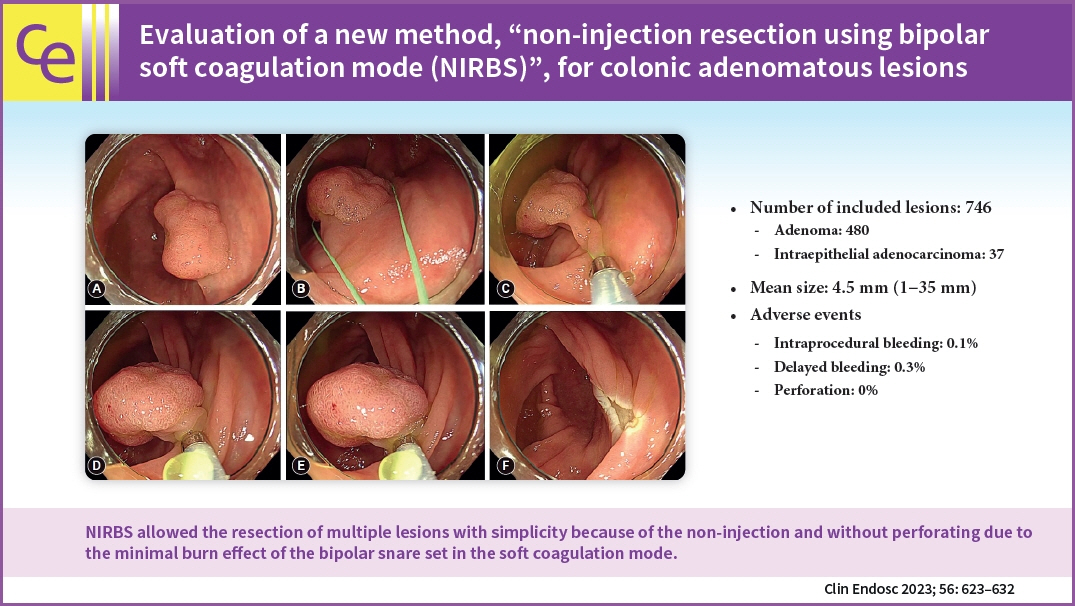
A total of 746 resected lesions were included in the study, with a 4.5 mm mean size (range, 1–35 mm). The major pathological breakdowns were as follows: 64.3% (480/746) were adenomas, and 5.0% (37/746) were intraepithelial adenocarcinomas (Tis lesions). No residuals were observed in any of the 37 Tis lesions (mean size, 15.3 mm). Adverse events included bleeding (0.4%) but no perforation.
Conclusions
NIRBS allowed the resection of multiple lesions with simplicity because of the non-injection and without perforating due to the minimal burn effect of the bipolar snare set in the soft coagulation mode. Therefore, NIRBS can be used to resect adenomatous lesions easily, including Tis lesions, from small to large lesions without leaving residuals.
Keyword
Figure
-
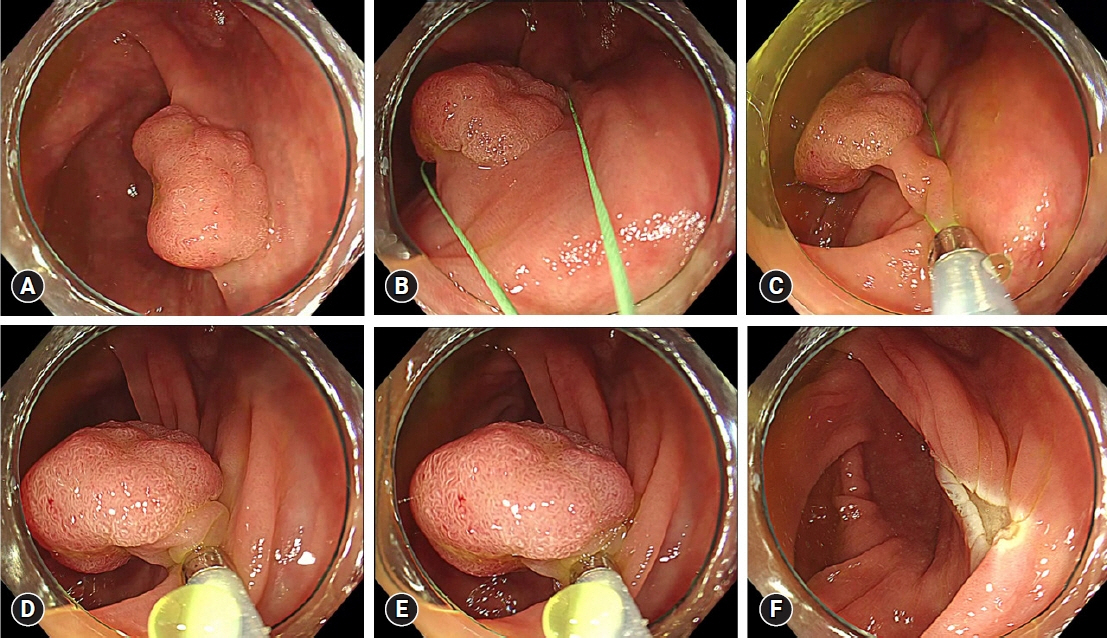
Fig. 1. Non-injection resection using bipolar soft coagulation mode procedure (NIRBS) Procedure 1. (A) Cecum, 20 mm, sessile type (Is). (B, C) The lesion is grasped by the snare, including the surrounding normal mucosa, while sucking air. (D) Grasped. (E) Squeezed and energized. (F) Resected.
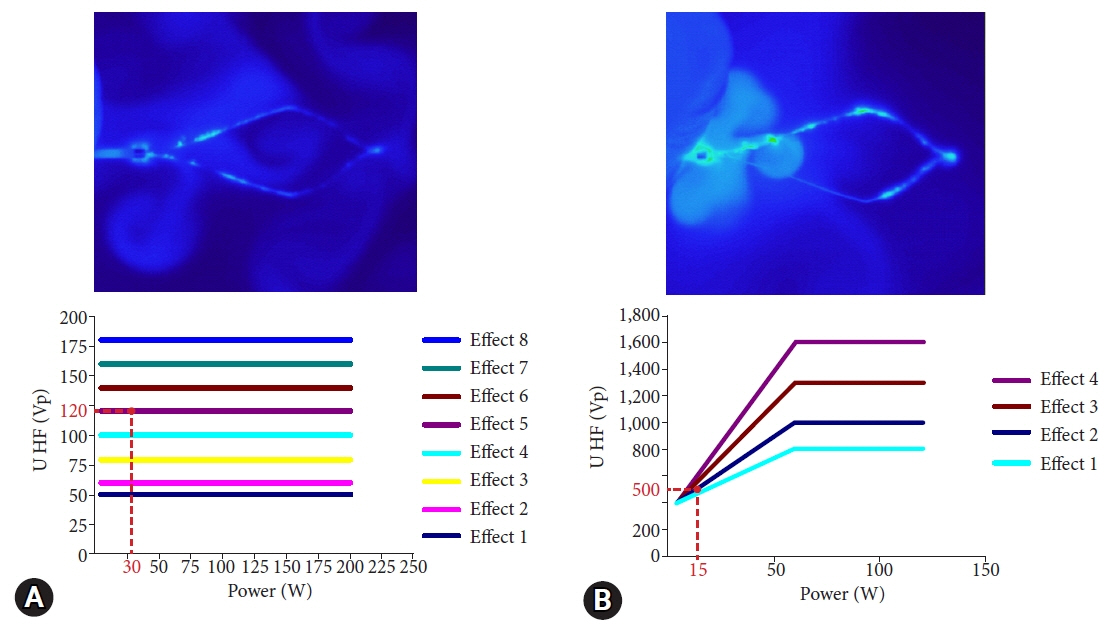
Fig. 2. Comparison between non-injection resection using bipolar soft coagulation mode (NIRBS) and the conventional bipolar forced coagulation mode. (A) NIRBS. (B) Conventional bipolar forced coagulation mode (forced, 15 W; effect 2). The thermographs of A and B were taken during energization by attaching the snare to the surface of the saline. The graphs (A) and (B) show the relationship between the electric power and voltage (the red number is the electric voltage in the mode). A comparison of the two thermographs shows that the NIRBS mode has less heat spread to the surface of saline than the conventional bipolar forced coagulation mode. A comparison of the two graphs shows that the electric voltage in the NIRBS mode is approximately 1/4 that in the conventional bipolar forced coagulation mode.
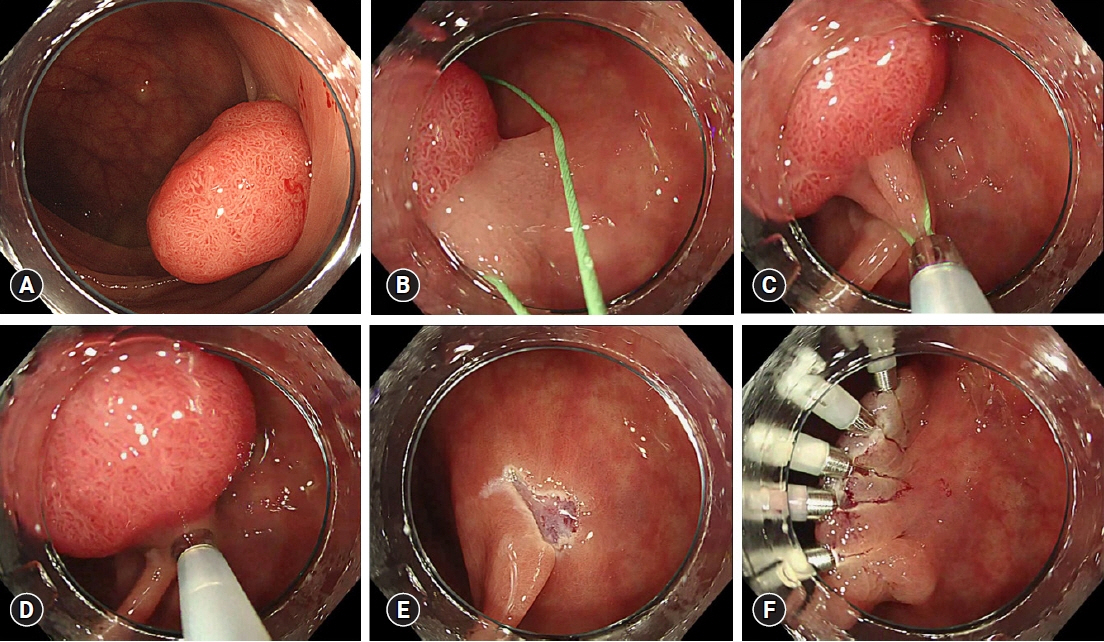
Fig. 3. Non-injection resection using bipolar soft coagulation mode procedure 2. (A) Sigmoid colon, 20 mm, semipedunculated type (Isp). (B, C) Snaring. (D) Grasped and squeezed. (E) Resected portion. (F) The resected portion was completely sutured with the clip because there were no mucosal swelling and minimal tissue solidification.
Reference
-
1. Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012; 366:687–696.2. Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood: Minnesota Colon Cancer Control Study. N Engl J Med. 1993; 328:1365–1371.3. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy: the National Polyp Study Workgroup. N Engl J Med. 1993; 329:1977–1981.4. Hardcastle JD, Chamberlain JO, Robinson MH, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996; 348:1472–1477.5. Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008; 134:1570–1595.6. Horiuchi A, Nakayama Y, Kajiyama M, et al. Removal of small colorectal polyps in anticoagulated patients: a prospective randomized comparison of cold snare and conventional polypectomy. Gastrointest Endosc. 2014; 79:417–423.7. Shinozaki S, Hayashi Y, Lefor AK, et al. What is the best therapeutic strategy for colonoscopy of colorectal neoplasia?: future perspectives from the East. Dig Endosc. 2016; 28:289–295.8. Rex DK, Bond JH, Winawer S, et al. Quality in the technical performance of colonoscopy and the continuous quality improvement process for colonoscopy: recommendations of the U.S. Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol. 2002; 97:1296–1308.9. Heldwein W, Dollhopf M, Rösch T, et al. The Munich Polypectomy Study (MUPS): prospective analysis of complications and risk factors in 4000 colonic snare polypectomies. Endoscopy. 2005; 37:1116–1122.10. Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc. 2015; 27:417–434.11. Ichise Y, Horiuchi A, Nakayama Y, et al. Prospective randomized comparison of cold snare polypectomy and conventional polypectomy for small colorectal polyps. Digestion. 2011; 84:78–81.12. Uraoka T, Ramberan H, Matsuda T, et al. Cold polypectomy techniques for diminutive polyps in the colorectum. Dig Endosc. 2014; 26 Suppl 2:98–103.13. Tutticci N, Burgess NG, Pellise M, et al. Characterization and significance of protrusions in the mucosal defect after cold snare polypectomy. Gastrointest Endosc. 2015; 82:523–528.14. Zhang Q, Gao P, Han B, et al. Polypectomy for complete endoscopic resection of small colorectal polyps. Gastrointest Endosc. 2018; 87:733–740.15. Kim JS, Lee BI, Choi H, et al. Cold snare polypectomy versus cold forceps polypectomy for diminutive and small colorectal polyps: a randomized controlled trial. Gastrointest Endosc. 2015; 81:741–747.16. Lee CK, Shim JJ, Jang JY. Cold snare polypectomy vs. cold forceps polypectomy using double-biopsy technique for removal of diminutive colorectal polyps: a prospective randomized study. Am J Gastroenterol. 2013; 108:1593–1600.17. Lee CK, Lee SH, Park JY, et al. Prophylactic argon plasma coagulation ablation does not decrease delayed postpolypectomy bleeding. Gastrointest Endosc. 2009; 70:353–361.18. Matsumoto M, Fukunaga S, Saito Y, et al. Risk factors for delayed bleeding after endoscopic resection for large colorectal tumors. Jpn J Clin Oncol. 2012; 42:1028–1034.19. Fujihara S, Mori H, Kobara H, et al. The efficacy and safety of prophylactic closure for a large mucosal defect after colorectal endoscopic submucosal dissection. Oncol Rep. 2013; 30:85–90.20. Burgess NG, Metz AJ, Williams SJ, et al. Risk factors for intraprocedural and clinically significant delayed bleeding after wide-field endoscopic mucosal resection of large colonic lesions. Clin Gastroenterol Hepatol. 2014; 12:651–661.21. Turan AS, Moons LM, Schreuder RM, et al. Clip placement to prevent delayed bleeding after colonic endoscopic mucosal resection (CLIPPER): study protocol for a randomized controlled trial. Trials. 2021; 22:63.22. Muniraj T, Sahakian A, Ciarleglio MM, et al. Cold snare polypectomy for large sessile colonic polyps: a single-center experience. Gastroenterol Res Pract. 2015; 2015:175959.23. Hirose R, Yoshida N, Murakami T, et al. Histopathological analysis of cold snare polypectomy and its indication for colorectal polyps 10-14 mm in diameter. Dig Endosc. 2017; 29:594–601.24. Kawamura T, Takeuchi Y, Asai S, et al. A comparison of the resection rate for cold and hot snare polypectomy for 4-9 mm colorectal polyps: a multicentre randomised controlled trial (CRESCENT study). Gut. 2018; 67:1950–1957.25. Shinozaki S, Kobayashi Y, Hayashi Y, et al. Efficacy and safety of cold versus hot snare polypectomy for resecting small colorectal polyps: systematic review and meta-analysis. Dig Endosc. 2018; 30:592–599.26. Qu J, Jian H, Li L, et al. Effectiveness and safety of cold versus hot snare polypectomy: a meta-analysis. J Gastroenterol Hepatol. 2019; 34:49–58.27. Kawamura T, Takeuchi Y, Yokota I, et al. Indications for cold polypectomy stratified by the colorectal polyp size: a systematic review and meta-analysis. J Anus Rectum Colon. 2020; 4:67–78.28. Ferlitsch M, Moss A, Hassan C, et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2017; 49:270–297.29. Shaukat A, Kaltenbach T, Dominitz JA, et al. Endoscopic recognition and management strategies for malignant colorectal polyps: recommendations of the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2020; 159:1916–1934.30. Sakamoto T, Matsuda T, Nakajima T, et al. Clinicopathological features of colorectal polyps: evaluation of the ‘predict, resect and discard’ strategies. Colorectal Dis. 2013; 15:e295–e300.31. Williams CB, de Peyer RC. Bipolar snare polypectomy: a safer technique for electrocoagulation of large polyp stalks. Endoscopy. 1979; 11:47–50.32. Tucker RD, Platz CE, Sievert CE, et al. In vivo evaluation of monopolar versus bipolar electrosurgical polypectomy snares. Am J Gastroenterol. 1990; 85:1386–1390.33. Shinmura K, Ikematsu H, Kojima M, et al. Safety of endoscopic procedures with monopolar versus bipolar instruments in an ex vivo porcine model. BMC Gastroenterol. 2020; 20:27.34. Saraya T, Ikematsu H, Fu KI, et al. Evaluation of complications related to therapeutic colonoscopy using the bipolar snare. Surg Endosc. 2012; 26:533–540.35. Sakuragi T, Okazaki Y, Mitsuoka M, et al. Dramatic hemostasis of the transected pulmonary artery model using SOFT COAG electrosurgical output. Interact Cardiovasc Thorac Surg. 2008; 7:764–766.36. Sakuragi T, Ohma H, Ohteki H. Efficacy of SOFT COAG for intraoperative bleeding in thoracic surgery. Interact Cardiovasc Thorac Surg. 2009; 9:767–768.37. Dumoulin FL, Hildenbrand R. Endoscopic resection techniques for colorectal neoplasia: current developments. World J Gastroenterol. 2019; 25:300–307.38. Law KE, Lowndes BR, Kelley SR, et al. Surgeon workload in colorectal surgery: perceived drivers of procedural difficulty. J Surg Res. 2020; 245:57–63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Monopolar and Bipolar Electrocoagulation in Brain
- The Effect of Monopolar and Bipolar Electrocoagulation in Spinal Cord
- Cervical conization with endoCUT mode applying gastrointestinal endoscopic polypectomy technique
- A Case of Endoscopic Resection of a Colonic Semipedunculated Leiomyoma
- A Case of a Colonic Giant Lipoma Removed by Endoscopic Resection
