Letter to the Editor : Classifying the Anatomical Location of the Ureter after Retroperitoneal Dissection
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea
- 2Department of Neurosurgery, School of Medicine, Pusan National University, Yangsan, Korea
- KMID: 2545352
- DOI: http://doi.org/10.3340/jkns.2023.0148
Figure
-
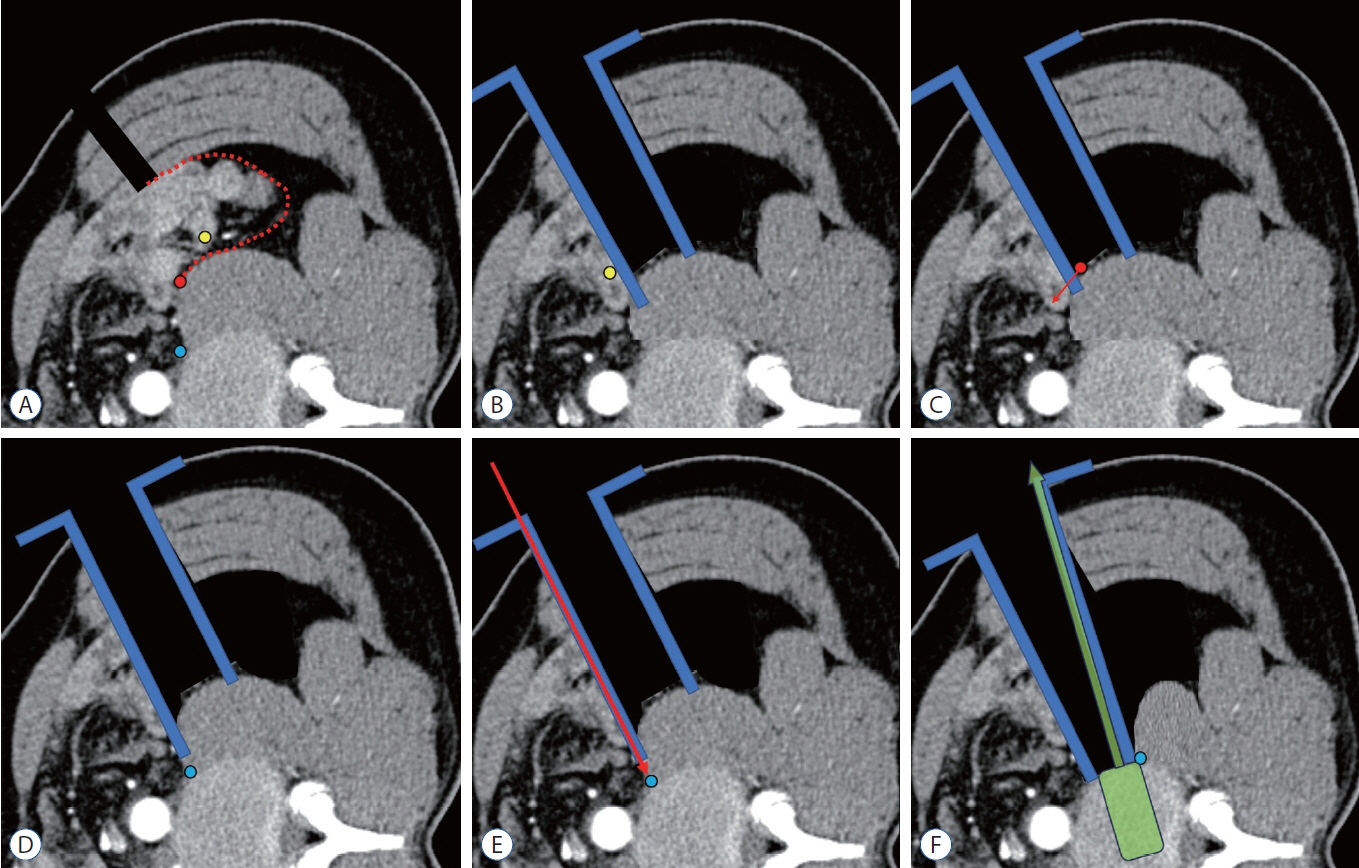
Fig. 1. Schematic location of the ureter on a dual-phase computed tomography scan. A : On the psoas (red circle), above the psoas (yellow circle), beside the psoas muscle (blue circle), retroperitoneal dissection plane (red dotted line). B : The ureter located above the psoas (yellow circle); after retroperitoneal dissection, the ureter can be easily retracted medially, retractor (blue). C : The ureter located on the psoas (red circle); after retroperitoneal dissection, the ureter can be easily visible and retracted medially (red arrow). D : The ureter is beside the psoas (blue circle); it is not identified even after conventional retroperitoneal dissection. E : The ureter can be injured by blindly fixing the retractor pinning (red arrow), or (F) blindly retracting the ureter laterally and injuring it during pull-out trials (green).
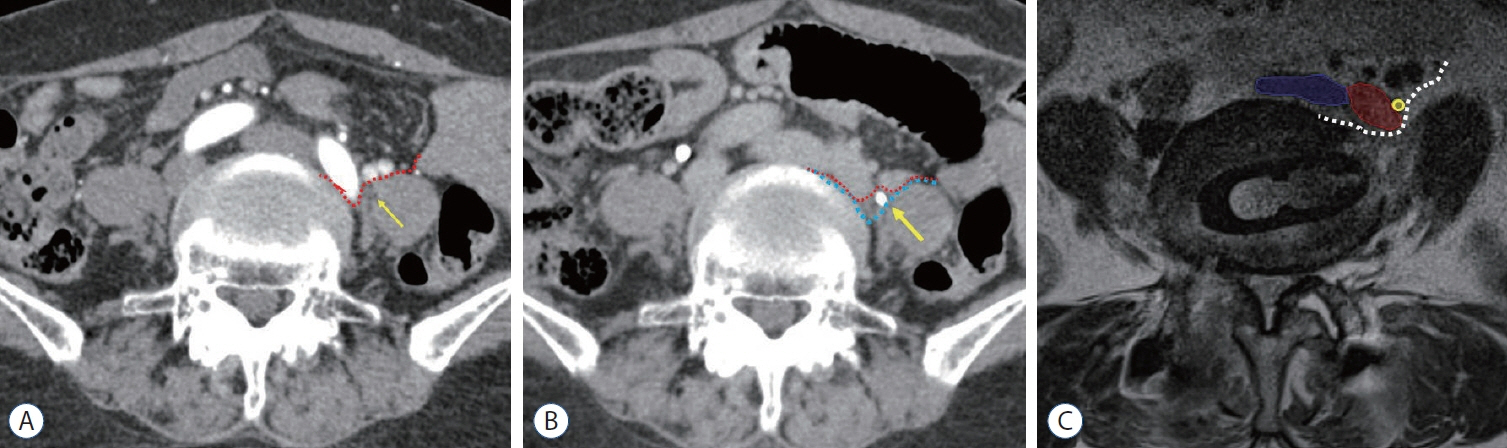
Fig. 2. Ureter under the psoas muscle. A and B : Preoperative dual phase computed tomography image (A : artery phase). The ureter (yellow arrow) cannot be distinguished from the psoas muscle, the retroperitoneal dissection plane is expected as a red dotted line (B : ureter phase). The left ureter (yellow arrow) hidden under the psoas muscle is contrast enhanced. To prevent ureter damage, identifying the ureter and medial retraction is necessary as the blue dotted line, (C) postoperative 1 week magnetic resonance imaging, left iliac vein and ureter and some visceral vessel was moved medially, white dotted line indicate the real dissection plane. Blue area : inferior vena cava, red area : left iliac artery, yellow circle : ureter.
Reference
-
References
1. Abe K, Orita S, Mannoji C, Motegi H, Aramomi M, Ishikawa T, et al. Perioperative complications in 155 patients who underwent oblique lateral interbody fusion surgery: perspectives and indications from a retrospective, multicenter survey. Spine (Phila Pa 1976). 42:55–62. 2017.2. Bjurlin MA, Rousseau LA, Vidal PP, Hollowell CM. Iatrogenic ureteral injury secondary to a thoracolumbar lateral revision instrumentation and fusion. Spine J. 9:e13–e15. 2009.3. Fujibayashi S, Otsuki B, Kimura H, Tanida S, Masamoto K, Matsuda S. Preoperative assessment of the ureter with dual-phase contrastenhanced computed tomography for lateral lumbar interbody fusion procedures. J Orthop Sci. 22:420–424. 2017.4. Huang C, Bian Z, Zhu L. Morphometric analysis of the ureter with respect to lateral lumbar interbody fusion using contrast-enhanced computed tomography. J Korean Neurosurg Soc. 66:155–161. 2023.5. Kim H, Chang BS, Chang SY. Pearls and pitfalls of oblique lateral interbody fusion: a comprehensive narrative review. Neurospine. 19:163–176. 2022.6. Kubota G, Orita S, Umimura T, Takahashi K, Ohtori S. Insidious intraoperative ureteral injury as a complication in oblique lumbar interbody fusion surgery: a case report. BMC Res Notes. 10:193. 2017.7. Lee HJ, Kim JS, Ryu KS, Park CK. Ureter injury as a complication of oblique lumbar interbody fusion. World Neurosurg. 102:693.e7–693.e14. 2017.8. Lee KH, Son DW, Oh BK, Lee SH, Lee JS, Kim YH, et al. Incidental ureteral complication in single-center consecutive oblique lateral interbody fusion cases. Turk Neurosurg. 2023; [Epub ahead of print].9. Lee YS, Lee DH, Cho DC, Han I, Kim CH, Kwon HD, et al. The change of spinal canal according to oblique lumbar interbody fusion in degenerative spondylolisthesis: a prospective observational study. Neurospine. 19:492–500. 2022.10. Oh BK, Son DW, Lee SH, Lee JS, Sung SK, Lee SW, et al. Learning curve and complications experience of oblique lateral interbody fusion : a single-center 143 consecutive cases. J Korean Neurosurg Soc. 64:447–459. 2021.11. Ouchida J, Kanemura T, Satake K, Nakashima H, Segi N. Anatomic evaluation of retroperitoneal organs for lateral approach surgery: a prospective imaging study using computed tomography in the lateral decubitus position. Eur Spine J. 28:835–841. 2019.12. Park SJ, Hwang JM, Cho DC, Lee S, Kim CH, Han I, et al. Indirect decompression using oblique lumbar interbody fusion revision surgery following previous posterior decompression: comparison of clinical and radiologic outcomes between direct and indirect decompression revision surgery. Neurospine. 19:544–554. 2022.13. Quillo-Olvera J, Lin GX, Jo HJ, Kim JS. Complications on minimally invasive oblique lumbar interbody fusion at L2-L5 levels: a review of the literature and surgical strategies. Ann Transl Med. 6:101. 2018.14. Son D, Lee S. Oblique Lumbar Interbody Fusion (OLIF) in Ahn Y, Park JK, Park CK (eds). Core Techniques of Minimally Invasive Spine Surgery. Singapore: Springer;2023. p. 243–265.15. Yingsakmongkol W, Jitpakdee K, Kerr S, Limthongkul W, Kotheeranurak V, Singhatanadgige W. Successful criteria for indirect decompression with lateral lumbar interbody fusion. Neurospine. 19:805–815. 2022.16. Yoon SG, Kim MS, Kwon SC, Lyo IU, Sim HB. Delayed ureter stricture and kidney atrophy after oblique lumbar interbody fusion. World Neurosurg. 134:137–140. 2020.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ureteral Stricture from Retroperitoneal Fibrosis Caused by Isolated Common Iliac Artery Aneurysm
- Morphometric Analysis of the Ureter with Respect to Lateral Lumbar Interbody Fusion Using Contrast-Enhanced Computed Tomography
- A Case of Unilateral Pelvic Kidney contained a Calculus
- Manufacture of the Serially Sectioned Images of the Whole Body (Fifth Report: Methods for Manufacture of the Three Dimensional Images and Virtual Dissection Software)
- Letter from Editor
