Paradigm Shift in Management of Hyperglycemia in Patients with Type 2 Diabetes: Glucocentric versus Organ Protection
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Sanggye Paik Hospital, Inje University School of Medicine, Seoul, Korea
- KMID: 2544517
- DOI: http://doi.org/10.4093/jkd.2023.24.2.59
Abstract
- The first research for managing patients with type 2 diabetes (T2DM) was the UK Prospective Diabetes Study. Subsequent studies have investigated the effects of intensive glucose control on diabetes-associated morbidities and mortality. Study results were intended to change a paradigm to control glycated hemoglobin and prevent diabetes-associated complications, but limited in microvascular diseases rather than diabetes-associated cardio-renal diseases and deaths. Comprehensive management of risk factors other than hyperglycemia (hypertension, dyslipidemia, chronic kidney disease) was emphasized to prevent atherosclerotic cardiovascular (CV) diseases and end-stage renal disease in T2DM. Since 2008, based clinical trials demonstrating CV safety, sodium-glucose transporter 2 inhibitors or glucagon-like peptide-1 receptor agonists have shown beneficial effects on macrovascular and renal complications in patients with T2DM. A recent new paradigm of diabetes care focuses on cardio-renal outcome-oriented care, namely organ-protection, instead of the typical glucocentric view endorsed by major societies across the world including the Korean Diabetes Association and disseminated into clinical practice even in primary care. Although there are many mechanisms by which those glucose-lowering agents protect CV and renal disease in patients with T2DM to be clarified, it is time to redefine diabetes care and to verify the CV effect of anti-diabetic medications beyond glucose lowering.
Keyword
Figure
-
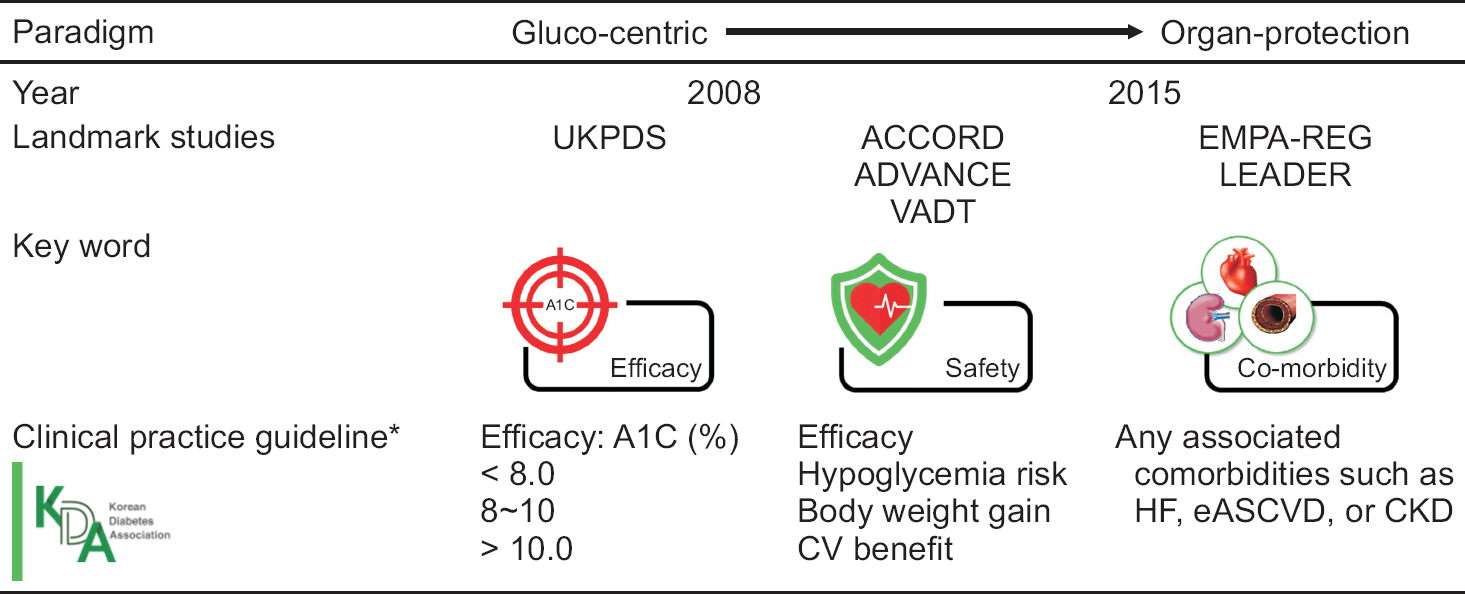
Fig. 1 Paradigm shift of diabetes care from glucocentric to organ-protection. UKPDS, UK Prospective Diabetes Study; ACCORD, Action to Control Cardiovascular Risk in Diabetes; ADVANCE, Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation; VADT, Veterans Affairs Diabetes Trial; EMPA-REG, Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients-Removing Excess Glucose; LEADER, Liraglutide Effect and Action in Diabetes; A1C, glycated hemoglobin; CV, cardiovascular; HF, heart failure; eASCVD, established atherosclerotic cardiovascular disease; CKD, chronic kidney disease. *Major recommendations for choosing a glucose-lowering agent after diabetes education for lifestyle modification and initial treatment with metformin otherwise severe hyperglycemia in 2007, 2011, and 2021 (from left to right, Ko et al. [12], Ko et al. [23], and Hur et al. [29], respectively).
Reference
-
1.Powers AC., Fowler MJ., Rickels MR. Diabetes mellitus: management and therapies. Loscalzo J, Fauci A, Kasper D, Hauser S, Longo D, Jameson JL, editors. Harrison's principles of internal medicine. 21st ed.New York, NY: McGraw Hill;2022.2.Di Angelantonio E., Gao P., Khan H., Butterworth AS., Wormser D., Kaptoge S, et al. Glycated hemoglobin mea-surement and prediction of cardiovascular disease. JAMA. 2014. 311:1225–33.
Article3.UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998. 352:837–53. Erratum in: Lancet 1999;354: 602.4.Stratton IM., Adler AI., Neil HA., Matthews DR., Manley SE., Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000. 321:405–12.
Article5.Pirart J. Diabetes mellitus and its degenerative complications: a prospective study of 4,400 patients observed between 1947 and 1973. Diabetes Care. 1978. 1:252–63.
Article6.World Health Organization (WHO). Use of glycated hae-moglobin (HbA1c) in diagnosis of diabetes mellitus: ab-breviated report of a WHO consultation. Geneva: WHO;2011.7.Marx N., McGuire DK., Perkovic V., Woerle HJ., Broedl UC., von Eynatten M, et al. Composite primary end points in cardiovascular outcomes trials involving type 2 diabetes patients: should unstable angina be included in the primary end point? Diabetes Care. 2017. 40:1144–51.
Article8.Holman RR., Paul SK., Bethel MA., Matthews DR., Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008. 359:1577–89.
Article9.Stratton IM., Cull CA., Adler AI., Matthews DR., Neil HA., Holman RR. Additive effects of glycaemia and blood pres-sure exposure on risk of complications in type 2 diabetes: a prospective observational study (UKPDS 75). Diabeto-logia. 2006. 49:1761–9.
Article10.Haffner SM. The Scandinavian Simvastatin Survival Study (4S) subgroup analysis of diabetic subjects: implications for the prevention of coronary heart disease. Diabetes Care. 1997. 20:469–71.
Article11.Gaede P., Lund-Andersen H., Parving HH., Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008. 358:580–91.
Article12.Ko SH., Kim SR., Kim DJ., Oh SJ., Lee HJ., Shim KH, et al. 2011 Clinical practice guidelines for type 2 diabetes in Korea. Diabetes Metab J. 2011. 35:431–6. Erratum in: Diabetes Metab J 2011;35: 642.
Article13.Gerstein HC., Miller ME., Ismail-Beigi F., Largay J., Mc-Donald C., Lochnan HA., ACCORD Study Group, et al. Effects of intensive glycaemic control on ischaemic heart disease: analysis of data from the randomised, controlled ACCORD trial. Lancet. 2014. 384:1936–41.
Article14.Patel A., MacMahon S., Chalmers J., Neal B., Billot L., Woodward M, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008. 358:2560–72.
Article15.Duckworth W., Abraira C., Moritz T., Reda D., Emanuele N., Reaven PD., VADT Investigators, et al. Glucose control and vascular complications in veterans with type 2 diabetes. N Engl J Med. 2009. 360:129–39.
Article16.Currie CJ., Peters JR., Tynan A., Evans M., Heine RJ., Bracco OL, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet. 2010. 375:481–9.
Article17.Inzucchi SE., Bergenstal RM., Buse JB., Diamant M., Fer-rannini E., Nauck M, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015. 38:140–9.
Article18.U. S. Food and Drug Administration. Guidance for indus-try on diabetes mellitus-evaluating cardiovascular risk in new anti-diabetic therapies to treat type 2 diabetes. Silver Spring, MD: U. S. Food and Drug Administration;2008.19.Bae JH., Han KD., Ko SH., Yang YS., Choi JH., Choi KM, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J. 2022. 46:417–26.
Article20.Scirica BM., Bhatt DL., Braunwald E., Steg PG., Davidson J., Hirshberg B., SAVOR-TIMI 53 Steering Committee and Investigators, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013. 369:1317–26.
Article21.Scheen AJ. Cardiovascular effects of new oral glucose-low-ering agents: DPP-4 and SGLT-2 inhibitors. Circ Res. 2018. 122:1439–59.22.Sano M. Mechanism by which dipeptidyl peptidase-4 inhibitors increase the risk of heart failure and possible differences in heart failure risk. J Cardiol. 2019. 73:28–32.
Article23.Ko SH., Hur KY., Rhee SY., Kim NH., Moon MK., Park SO., Committee of Clinical Practice Guideline of Korean Diabetes Association, et al. Antihyperglycemic agent therapy for adult patients with type 2 diabetes mellitus 2017: a position statement of the Korean Diabetes Association. Diabetes Metab J. 2017. 41:337–48.
Article24.Kim GS., Park JH., Won JC. The role of glucagon-like pep-tide 1 receptor agonists and sodium-glucose cotransporter 2 inhibitors in reducing cardiovascular events in patients with type 2 diabetes. Endocrinol Metab (Seoul). 2019. 34:106–16.
Article25.Vaduganathan M., Januzzi JL Jr. Preventing and treating heart failure with sodium-glucose co-transporter 2 inhibitors. Am J Med. 2019. 132(10 Suppl):S21–9.
Article26.Home P. Controversies for glucose control targets in type 2 diabetes: exposing the common ground. Diabetes Care. 2019. 42:1615–23.
Article27.Heerspink HJL., Stefánsson BV., Correa-Rotter R., Chertow GM., Greene T., Hou FF., DAPA-CKD Trial Com-mittees and Investigators, et al. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020. 383:1436–46.
Article28.Ryan DH., Lingvay I., Colhoun HM., Deanfield J., Emerson SS., Kahn SE, et al. Semaglutide effects on cardiovascular outcomes in people with overweight or obesity (SELECT) rationale and design. Am Heart J. 2020. 229:61–9.
Article29.Hur KY., Moon MK., Park JS., Kim SK., Lee SH., Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J. 2021. 45:461–81.
Article30.Kibble JD., Halsey CR. Medical physiology: the big picture. New York, NY: McGraw Hill;2014. Notice.31.Banting FG., Best CH., Collip JB., Campbell WR., Fletcher AA. Pancreatic extracts in the treatment of diabetes mellitus. Can Med Assoc J. 1922. 12:141–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Summary: Management of Hyperglycemia in Type 2 Diabetes according to the 2022 ADA-EASD Consensus Report and 2023 ADA Standards of Care in Diabetes
- Pharmacotherapy for Postprandial Hyperglycemia in Type 2 Diabetes
- Comprehensive Management in Patients with Type 2 Diabetes Mellitus
- Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach Developed by the American Diabetes Association and the European Association for the Study of Diabetes
- The Role of Educational Nurses in Inpatient Management for Diabetes Care: 2023 ADA Practice Guidelines
