Computed tomography-based analysis of the characteristics of fifth metacarpal neck fractures and its clinical applications
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea University Anam Hospital, Seoul, Korea
- KMID: 2542558
- DOI: http://doi.org/10.12790/ahm.23.0006
Abstract
- Purpose
Understanding the configuration and characteristics of the comminuted fifth metacarpal neck fractures is essential for successful operative treatment, especially for antegrade intramedullary Kirchner wire (K-wire) fixation. This study aimed to investigate the characteristics and shape of comminuted fragments in fifth metacarpal neck fractures and suggest the appropriate K-wire position.
Methods
Forty-one cases of fifth metacarpal neck fractures operated from January 2010 to April 2022 were enrolled in this study. The length and width of the comminuted fragments were measured, as well as the distance from the articular surface of the fifth metacarpal head to the comminuted fragment (Da-c) and the distance from the articular surface to the proximal end of the metacarpal head (Da-h). The location of the comminuted fragments was categorized in terms of four quadrants: dorsal-ulnar (DU), dorsal-radial (DR), palmar-radial, and palmar-ulnar.
Results
Among 41 patients with fifth metacarpal neck fractures, comminuted fracture fragments were observed in 35 cases (85.4%). The mean length and width of the comminuted fragments were 7.5±2.3 mm and 3.2±0.8 mm, respectively. The comminuted fragments were on the dorsal aspect of the fracture in all cases; 27 (77.1%) in the DU quadrant and 8 (22.9%) in the DR quadrant. The mean Da-c and Da-h were 5.3±1.6 mm and 10.9±1.5 mm, respectively.
Conclusion
To ensure stable K-wire fixation, it is essential to identify the location and characteristics of the comminuted fracture fragments before surgery and subsequently choose an appropriate K-wire position.
Figure
-

Fig. 1. Measurements of the fracture profile. (A) The length and width of the comminuted fragments are measured on a coronal computed tomography (CT) scan. (B) The distance from the articular surface to the comminuted fragments (Da-c) and the distance from the articular surface to the proximal end of the metacarpal head (Da-h) are measured on a sagittal CT scan. (C) The location of the comminuted fragment is categorized according to four quadrants on an axial CT scan (dorsal-ulnar [DU], palmar-ulnar [PU], palmar-radial [PR], and dorsal-radial [DR]). (D) An example of a comminuted fragment located in the DU quadrant.

Fig. 2. The optimal positioning of Kirchner wires (K-wires) in antegrade intramedullary pinning. (A) The bent distal tip of a K-wire that goes to the dorsal-ulnar corner has a risk of perforation through the comminuted fragments and consequent fixation loss. (B) The bent distal tip of a K-wire positioned in the volar-radial corner of the metacarpal head provides stronger fixability.
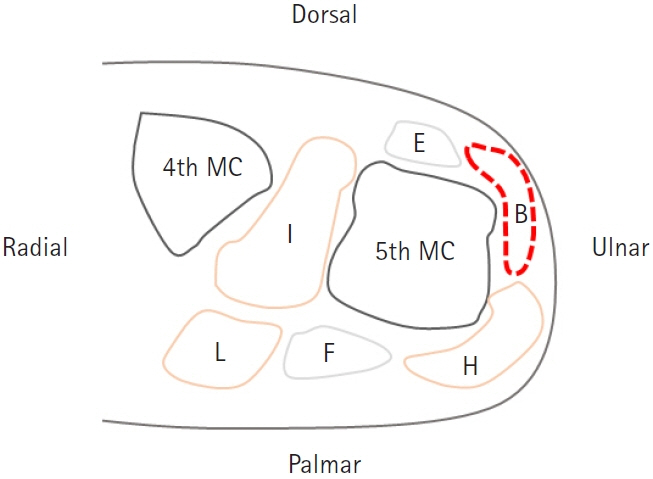
Fig. 3. Soft tissues surrounding the fifth metacarpal neck. E, extensors; I, interossei; L, lumbricals; F, flexors; H, hypothenar muscles; MC, metacarpal; B, bare area.
Reference
-
References
1. Feehan LM, Sheps SB. Incidence and demographics of hand fractures in British Columbia, Canada: a population-based study. J Hand Surg Am. 2006; 31:1068–74.
Article2. Nakashian MN, Pointer L, Owens BD, Wolf JM. Incidence of metacarpal fractures in the US population. Hand (N Y). 2012; 7:426–30.
Article3. Zong SL, Zhao G, Su LX, et al. Treatments for the fifth metacarpal neck fractures: a network meta-analysis of randomized controlled trials. Medicine (Baltimore). 2016; 95:e3059.4. Gudmundsen TE, Borgen L. Fractures of the fifth metacarpal. Acta Radiol. 2009; 50:296–300.
Article5. de Jonge JJ, Kingma J, van der Lei B, Klasen HJ. Fractures of the metacarpals: a retrospective analysis of incidence and aetiology and a review of the English-language literature. Injury. 1994; 25:365–9.
Article6. Soong M, Got C, Katarincic J. Ring and little finger metacarpal fractures: mechanisms, locations, and radiographic parameters. J Hand Surg Am. 2010; 35:1256–9.
Article7. Kollitz KM, Hammert WC, Vedder NB, Huang JI. Metacarpal fractures: treatment and complications. Hand (N Y). 2014; 9:16–23.
Article8. Padegimas EM, Warrender WJ, Jones CM, Ilyas AM. Metacarpal neck fractures: a review of surgical indications and techniques. Arch Trauma Res. 2016; 5:e32933.
Article9. Eisenschenk A, Spitzmüller R, Güthoff C, et al. Single versus dual Kirschner wires for closed reduction and intramedullary nailing of displaced fractures of the fifth metacarpal neck (1-2 KiWi): a randomized controlled trial. Bone Joint J. 2019; 101-B:1263–71.10. Rhee SH, Lee SK, Lee SL, Kim J, Baek GH, Lee YH. Prospective multicenter trial of modified retrograde percutaneous intramedullary Kirschner wire fixation for displaced metacarpal neck and shaft fractures. Plast Reconstr Surg. 2012; 129:694–703.
Article11. Amsallem L, Pierrart J, Bihel T, et al. Simplified internal fixation of fifth metacarpal neck fractures. Orthop Traumatol Surg Res. 2018; 104:257–60.
Article12. Kim JK, Kim DJ. Antegrade intramedullary pinning versus retrograde intramedullary pinning for displaced fifth metacarpal neck fractures. Clin Orthop Relat Res. 2015; 473:1747–54.
Article13. Galal S, Safwat W. Transverse pinning versus intramedullary pinning in fifth metacarpal's neck fractures: a randomized controlled study with patient-reported outcome. J Clin Orthop Trauma. 2017; 8:339–43.
Article14. Balaram AK, Bednar MS. Complications after the fractures of metacarpal and phalanges. Hand Clin. 2010; 26:169–77.
Article15. Mohammed R, Farook MZ, Newman K. Percutaneous elastic intramedullary nailing of metacarpal fractures: surgical technique and clinical results study. J Orthop Surg Res. 2011; 6:37.
Article16. Schädel-Höpfner M, Wild M, Windolf J, Linhart W. Antegrade intramedullary splinting or percutaneous retrograde crossed pinning for displaced neck fractures of the fifth metacarpal? Arch Orthop Trauma Surg. 2007; 127:435–40.
Article17. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016; 15:155–63.
Article18. Fusetti C, Meyer H, Borisch N, Stern R, Santa DD, Papaloïzos M. Complications of plate fixation in metacarpal fractures. J Trauma. 2002; 52:535–9.
Article19. Freeland AE, Orbay JL. Extraarticular hand fractures in adults: a review of new developments. Clin Orthop Relat Res. 2006; 445:133–45.20. Kelsch G, Ulrich C. Intramedullary k-wire fixation of metacarpal fractures. Arch Orthop Trauma Surg. 2004; 124:523–6.
Article21. Calder JD, O’Leary S, Evans SC. Antegrade intramedullary fixation of displaced fifth metacarpal fractures. Injury. 2000; 31:47–50.
Article22. Fricker R, Kastelec M, Nuñez F, Axelrod T. Intramedullary K-wire fixation for fifth metacarpal neck fracture [Internet]. Coton C, editor. AO Surgery Reference. [cited 2022 Aug 5]. Available from: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/metacarpals/head-subcapital/intramedullary-k-wire-fixation.23. Hussain MH, Ghaffar A, Choudry Q, Iqbal Z, Khan MN. Management of fifth metacarpal neck fracture (boxer's fracture): a literature review. Cureus. 2020; 12:e9442.
Article24. Chan K, Bhandari M. Three-minute critical appraisal of a case series article. Indian J Orthop. 2011; 45:103–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison between Two Kirschner Wire Fixation and Three Wire Fixation, in Treating of Metacarpal Neck Fracture Using Multiple Retrograde Kirschner Wire Fixation
- Antegrade Intramedullary Prebent K-wire Fixation for the 5th Metacarpal Neck Fracture
- The Treatment Outcomes of the Metacarpal Shaft and Neck Comminuted Fractures Using Modified Percutaneous Retrograde Intramedullary Kirschner Wire Fixation
- Avulsion Fracture of the Index Metacarpal Base: Two Case Reports
- Fractures of the Wrist and Hand after Punching Injury
