Acute Crit Care.
2022 Aug;37(3):407-414. 10.4266/acc.2022.00164.
The effects of hypomagnesemia on delirium in middle-aged and older adult patients admitted to medical intensive care units
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea
- KMID: 2535305
- DOI: http://doi.org/10.4266/acc.2022.00164
Abstract
- Background
In critically ill patients, the most common manifestation of brain dysfunction is delirium, which is independently associated with higher morbidity and mortality. While electrolyte imbalance is one of the precipitating factors, the impact of hypomagnesemia on the incidence of delirium remains unknown.
Methods
We retrospectively analyzed patients admitted to the medical intensive care unit (ICU) of a tertiary referral center between January and June 2020. Patients with ICU stay ≥48 hours and aged 40–85 years were included. The primary outcome was cumulative incidence of delirium in the ICU. Patients were divided into two groups based on serum magnesium level at ICU admission. Multivariable Cox proportional hazards regression analysis was performed, and covariates were selected using the least absolute shrinkage and selection operator (LASSO) method.
Results
A total of 109 patients included 43 (39.4%) women and had a median age of 69.0 years (interquartile range [IQR], 60.0–76.0 years). The median magnesium level was 1.7 mg/dl (IQR, 1.5–1.9 mg/dl), and the cumulative incidence of delirium was 32.1% (35 patients). Hypomagnesemia was independently associated with delirium (adjusted hazard ratio [aHR], 2.12; 95% confidence interval [CI], 1.03–4.38), along with prior use of immunosuppressants (aHR, 3.08; 95% CI, 1.46–6.48) or benzodiazepines (aHR, 4.02; 95% CI, 1.54–10.50), body mass index (aHR, 0.93; 95% CI, 0.84–1.02), and alcohol history (aHR, 1.68; 95% CI, 0.74–3.80).
Conclusions
In critically ill adults, hypomagnesemia increases the risk of delirium by more than two-fold compared to patients with normal magnesium level.
Keyword
Figure
-
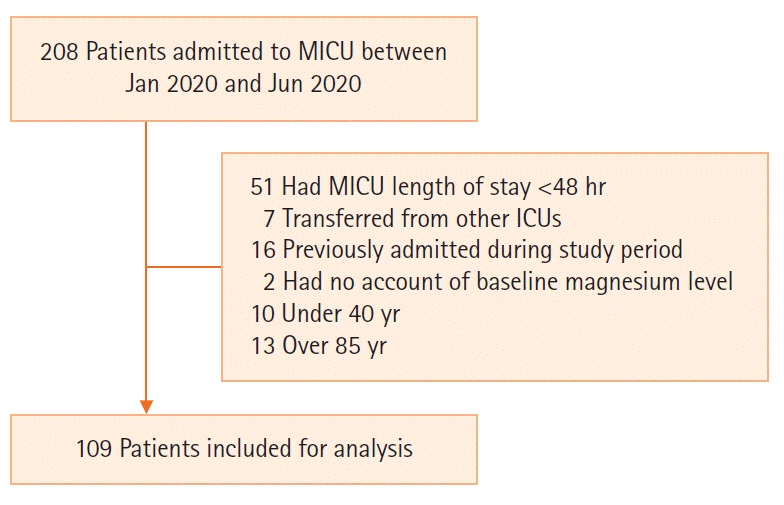
Figure 1. Flowchart of the patients included in the study. MICU: medical intensive care unit; ICU: intensive care unit.
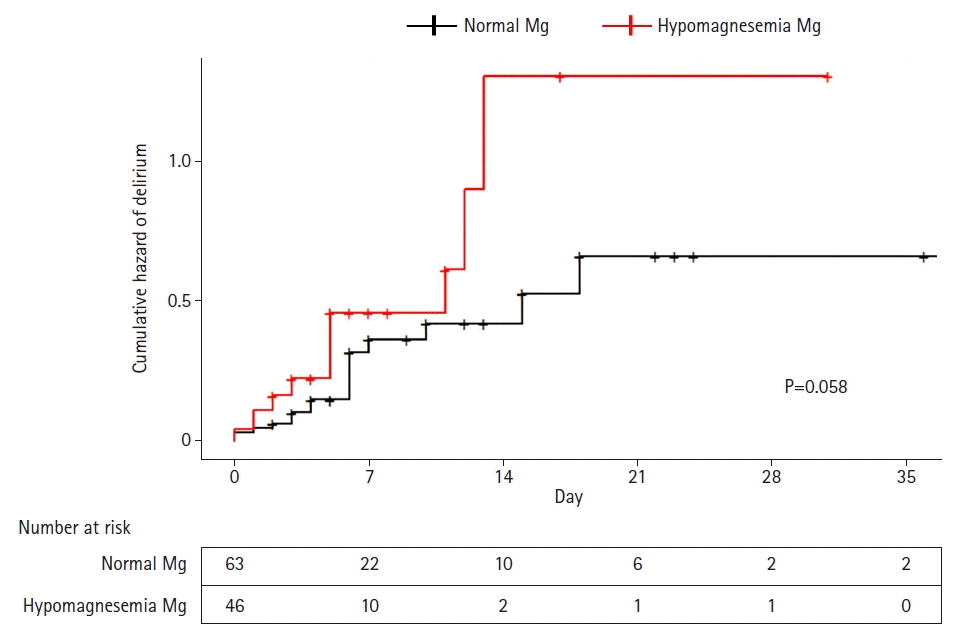
Figure 2. Cumulative hazard plot of delirium in the intensive care unit stratified by magnesium (Mg) level.
Reference
-
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. Washington (DC): American Psychiatric Association; 2013.2. Stollings JL, Kotfis K, Chanques G, Pun BT, Pandharipande PP, Ely EW. Delirium in critical illness: clinical manifestations, outcomes, and management. Intensive Care Med. 2021; 47:1089–03.3. Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE Jr, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004; 291:1753–62.4. Salluh JI, Wang H, Schneider EB, Nagaraja N, Yenokyan G, Damluji A, et al. Outcome of delirium in critically ill patients: systematic review and meta-analysis. BMJ. 2015; 350:h2538.5. Vasilevskis EE, Chandrasekhar R, Holtze CH, Graves J, Speroff T, Girard TD, et al. The cost of ICU delirium and coma in the intensive care unit patient. Med Care. 2018; 56:890–7.6. Lin SM, Liu CY, Wang CH, Lin HC, Huang CD, Huang PY, et al. The impact of delirium on the survival of mechanically ventilated patients. Crit Care Med. 2004; 32:2254–9.7. Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007; 33:66–73.8. Van Rompaey B, Elseviers MM, Schuurmans MJ, Shortridge-Baggett LM, Truijen S, Bossaert L. Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care. 2009; 13:R77.9. Sonneville R, de Montmollin E, Poujade J, Garrouste-Orgeas M, Souweine B, Darmon M, et al. Potentially modifiable factors contributing to sepsis-associated encephalopathy. Intensive Care Med. 2017; 43:1075–84.
Article10. Hong JH. Delirium in the intensive care unit. J Neurocrit Care. 2015; 8:46–52.
Article11. Zieschang T, Wolf M, Vellappallil T, Uhlmann L, Oster P, Kopf D. The Association of hyponatremia, risk of confusional state, and mortality. Dtsch Arztebl Int. 2016; 113:855–62.
Article12. Riggs JE. Neurologic manifestations of electrolyte disturbances. Neurol Clin. 2002; 20:227–39.
Article13. Shrimanker I, Bhattarai S. Electrolytes. Treasure Island: StatPearls Publishing;2021.14. Cirik MÖ, Kilinç M, Doğanay GE, Ünver M, Yildiz M, Avci S. The relationship between magnesium levels and mortality in the respiratory intensive care unit. Medicine (Baltimore). 2020; 99:e23290.
Article15. Panahi Y, Mojtahedzadeh M, Najafi A, Ghaini MR, Abdollahi M, Sharifzadeh M, et al. The role of magnesium sulfate in the intensive care unit. EXCLI J. 2017; 16:464–82.16. Fairley J, Glassford NJ, Zhang L, Bellomo R. Magnesium status and magnesium therapy in critically ill patients: a systematic review. J Crit Care. 2015; 30:1349–58.
Article17. Karnik ND, Gupta AV. Hypomagnesemia in ICU. J Assoc Physicians India. 2016; 64:11–3.18. Noronha JL, Matuschak GM. Magnesium in critical illness: metabolism, assessment, and treatment. Intensive Care Med. 2002; 28:667–79.
Article19. Lee HJ, Bae E, Lee HY, Lee SM, Lee J. Association of natural light exposure and delirium according to the presence or absence of windows in the intensive care unit. Acute Crit Care. 2021; 36:332–41.
Article20. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990; 113:941–8.
Article21. Lindner G, Funk GC. Hypernatremia in critically ill patients. J Crit Care. 2013; 28:216.e11–20.
Article22. Cao Y, Zhen S, Taylor AW, Appleton S, Atlantis E, Shi Z. Magnesium Intake and sleep disorder symptoms: findings from the Jiangsu nutrition study of Chinese adults at five-year follow-up. Nutrients. 2018; 10:1354.
Article23. Kumar S, Jain S, Agrawal S, Honmode A. Impact of serum magnesium levels in critically ill elderly patients: a study in a rural teaching hospital. J Clin Gerontol Geriatr. 2016; 7:104–8.24. Dorhout Mees SM, Algra A, Vandertop WP, van Kooten F, Kuijsten HA, Boiten J, et al. Magnesium for aneurysmal subarachnoid haemorrhage (MASH-2): a randomised placebo-controlled trial. Lancet. 2012; 380:44–9.
Article25. Saver JL, Starkman S, Eckstein M, Stratton SJ, Pratt FD, Hamilton S, et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. N Engl J Med. 2015; 372:528–36.
Article26. Altun D, Eren G, Cetingok H, Hergünsel GO, Çukurova Z. Can we use magnesium for sedation in the intensive care unit for critically ill patients: is it as effective as other sedatives? Agri. 2019; 31:86–92.27. Limaye CS, Londhey VA, Nadkart MY, Borges NE. Hypomagnesemia in critically ill medical patients. J Assoc Physicians India. 2011; 59:19–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effects of Delirium Care Training Program for Nurses in Hospital Nursing Units
- Intensive Care Unit Nurse's Knowledge, Nursing Performance, and Stress about Delirium
- Delirium in the intensive care unit
- Prevalence and risk factors of delirium of older adults after cardiac surgery at the intensive care unit: A retrospective study
- Investigation of Delirium Occurrence and Intervention Status in Intensive Care Unit at a Hospital and Perception of Delirium by Medical Staff
