Child Kidney Dis.
2022 Jun;26(1):58-62. 10.3339/ckd.22.024.
Recurrent hemolytic uremic syndrome caused by DGKE gene mutation: a case report
- Affiliations
-
- 1Department of Pediatrics, Seoul National University Children's Hospital, Seoul, Republic of Korea
- 2Department of Pediatrics, Seoul National University College of Medicine, Seoul, Republic of Korea
- 3Kidney Research Institute, Medical Research Center, Seoul National University College of Medicine, Seoul, Republic of Korea
- 4Wide River Institute of Immunology, Seoul National University, Hongcheon, Republic of Korea
- KMID: 2531936
- DOI: http://doi.org/10.3339/ckd.22.024
Abstract
- Atypical hemolytic uremic syndrome (aHUS) is a rare disease characterized by microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury without any association with preceding diarrhea. Dysregulation of the complement system is the most common cause of aHUS, and monoclonal humanized anti-C5 antibodies are now recommended as the first-line treatment for aHUS. However, if the complement pathway is not the cause of aHUS, C5 inhibitors are ineffective. In this study, we report the second reported case of aHUS caused by DGKE mutations in Republic of Korea. The patient was an 11-month-old infant who presented with prodromal diarrhea similar to typical HUS, self-remitted with conservative management unlike complement-mediated aHUS but recurred with fever. While infantile aHUS often implies genetic dysregulation of the complement system, other rare genetic causes, such as DGKE mutation, need to be considered before deciding long-term treatment with C5 inhibitors.
Figure
-
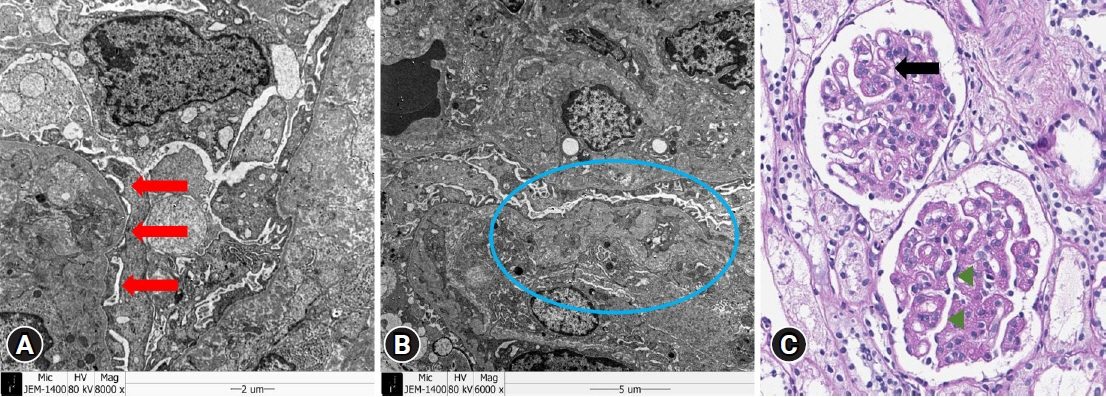
Fig. 1. Pathologic findings. (A) Electron microscopy image. Diffuse thickened glomerular basement membrane and focal slight effacement of foot process were marked with red arrows. (B) Electron microscopy image. Subendothelial widening and mesangial interposition were marked with blue circle. (C) Periodic acid-Schiff staining image (×500). Endothelial cells were mildly hypercellular in the glomerulus and glomerular size was mildly increased (marked with black arrow). Some glomerulus showed tram-track appearance (marked with green arrowheads).
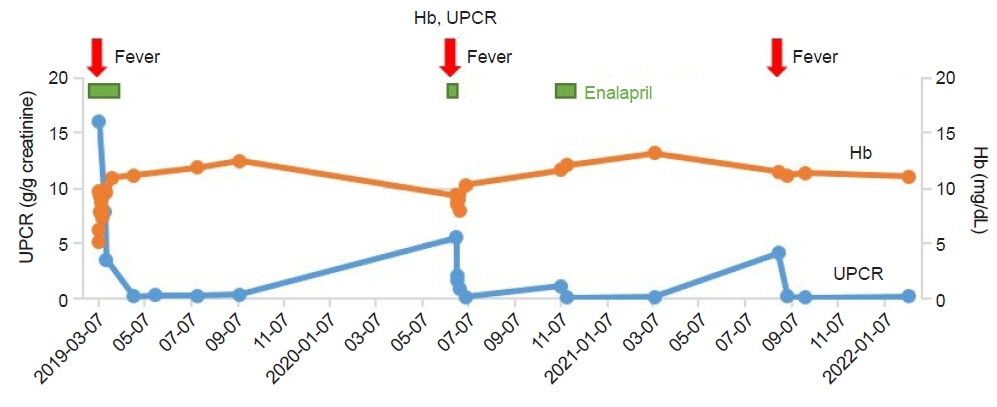
Fig. 2. Laboratory data. Fever events are annotated with red arrows. Hb, hemoglobin; UPCR, urine protein/creatinine ratio.
Reference
-
References
1. Loirat C, Noris M, Fremeaux-Bacchi V. Complement and the atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2008; 23:1957–72.
Article2. Geerdink LM, Westra D, van Wijk JA, Dorresteijn EM, Lilien MR, Davin JC, et al. Atypical hemolytic uremic syndrome in children: complement mutations and clinical characteristics. Pediatr Nephrol. 2012; 27:1283–91.
Article3. Loirat C, Fakhouri F, Ariceta G, Besbas N, Bitzan M, Bjerre A, et al. An international consensus approach to the management of atypical hemolytic uremic syndrome in children. Pediatr Nephrol. 2016; 31:15–39.
Article4. McNamara LA, Topaz N, Wang X, Hariri S, Fox L, MacNeil JR. High risk for invasive meningococcal disease among patients receiving eculizumab (Soliris) despite receipt of meningococcal vaccine. MMWR Morb Mortal Wkly Rep. 2017; 66:734–7.
Article5. Nester CM, Thomas CP. Atypical hemolytic uremic syndrome: what is it, how is it diagnosed, and how is it treated? Hematology Am Soc Hematol Educ Program. 2012; 2012:617–25.
Article6. Lee JM, Park YS, Lee JH, Park SJ, Shin JI, Park YH, et al. Atypical hemolytic uremic syndrome: Korean pediatric series. Pediatr Int. 2015; 57:431–8.
Article7. Lemaire M, Fremeaux-Bacchi V, Schaefer F, Choi M, Tang WH, Le Quintrec M, et al. Recessive mutations in DGKE cause atypical hemolytic-uremic syndrome. Nat Genet. 2013; 45:531–6.
Article8. Bezdicka M, Pavlicek P, Blahova K, Hacek J, Zieg J. Various phenotypes of disease associated with mutated DGKE gene. Eur J Med Genet. 2020; 63:103953.9. Azukaitis K, Simkova E, Majid MA, Galiano M, Benz K, Amann K, et al. The phenotypic spectrum of nephropathies associated with mutations in diacylglycerol kinase ε. J Am Soc Nephrol. 2017; 28:3066–75.10. Mele C, Lemaire M, Iatropoulos P, Piras R, Bresin E, Bettoni S, et al. Characterization of a new DGKE intronic mutation in genetically unsolved cases of familial atypical hemolytic uremic syndrome. Clin J Am Soc Nephrol. 2015; 10:1011–9.11. Noris M, Remuzzi G. Atypical hemolytic-uremic syndrome. N Engl J Med. 2009; 361:1676–87.
Article12. Husain D, Barron B, Barron AG, Sandokji I, Marsenic O, Warejko JK. Atypical hemolytic uremic syndrome due to DGKE mutation and response to eculizumab: lessons for the clinical nephrologist. J Nephrol. 2021; 34:1331–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of the Diarrhea-associated Hemolytic Uremic Syndrome Developing Simultaneously with an Acute Appendicitis
- A clinical aspect of the hemolytic uremic syndrome
- A Case of Microangiopathic Hemolytic Anemia after Myxoma Excision and Mitral Valve Repair Presenting as Hemolytic Uremic Syndrome
- Cyclosporin-A associated hemolytic-uremic syndrome in renalallograft recipient: a case report
- A case of recurrent postpartum hemolytic uremic syndrome
