Clinical Significance of Additional Ablation of Atrial Premature Beats after Catheter Ablation for Atrial Fibrillation
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University Health System, Seoul, Korea. hnpak@yuhs.ac
- KMID: 2466354
- DOI: http://doi.org/10.3349/ymj.2016.57.1.72
Abstract
- PURPOSE
The clinical significance of post-procedural atrial premature beats immediately after catheter ablation for atrial fibrillation (AF) has not been clearly determined. We hypothesized that the provocation of immediate recurrence of atrial premature beats (IRAPB) and additional ablation improves the clinical outcome of AF ablation.
MATERIALS AND METHODS
We enrolled 200 patients with AF (76.5% males; 57.4+/-11.1 years old; 64.3% paroxysmal AF) who underwent catheter ablation. Post-procedure IRAPB was defined as frequent atrial premature beats (> or =6/min) under isoproterenol infusion (5 microg/min), monitored for 10 min after internal cardioversion, and we ablated mappable IRAPBs. Post-procedural IRAPB provocations were conducted in 100 patients. We compared the patients who showed IRAPB with those who did not. We also compared the IRAPB provocation group with 100 age-, sex-, and AF-type-matched patients who completed ablation without provocation (No-Test group).
RESULTS
1) Among the post-procedural IRAPB provocation group, 33% showed IRAPB and required additional ablation with a longer procedure time (p=0.001) than those without IRAPB, without increasing the complication rate. 2) During 18.0+/-6.6 months of follow-up, the patients who showed IRAPB had a worse clinical recurrence rate than those who did not (27.3% vs. 9.0%; p=0.016), in spite of additional IRAPB ablation. 3) However, the clinical recurrence rate was significantly lower in the IRAPB provocation group (15.0%) than in the No-Test group (28.0%; p=0.025) without lengthening of the procedure time or raising complication rate.
CONCLUSION
The presence of post-procedural IRAPB was associated with a higher recurrence rate after AF ablation. However, IRAPB provocation and additional ablation might facilitate a better clinical outcome. A further prospective randomized study is warranted.
MeSH Terms
Figure
-
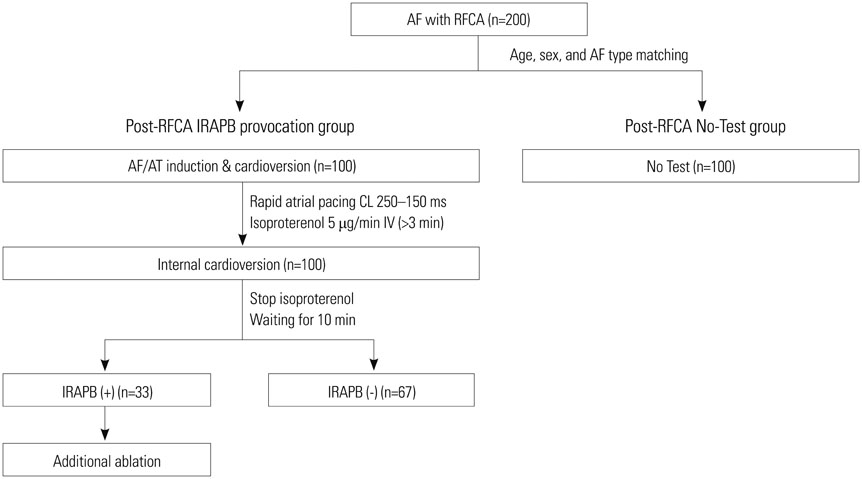
Fig. 1 Diagram of study protocol. We compared the clinical efficacy of post-procedural provocation for immediate recurrence of atrial premature beats (IRAPBs) under isoproterenol and additional ablation targeting these APBs (n=100) with 100 age-, sex-, and AF-type-matched patients who completed the procedure without an induction test (No-Test group). CL, cycle length; RFCA, radiofrequency catheter ablation; AF, atrial fibrillation; AT, atrial tachycardia.
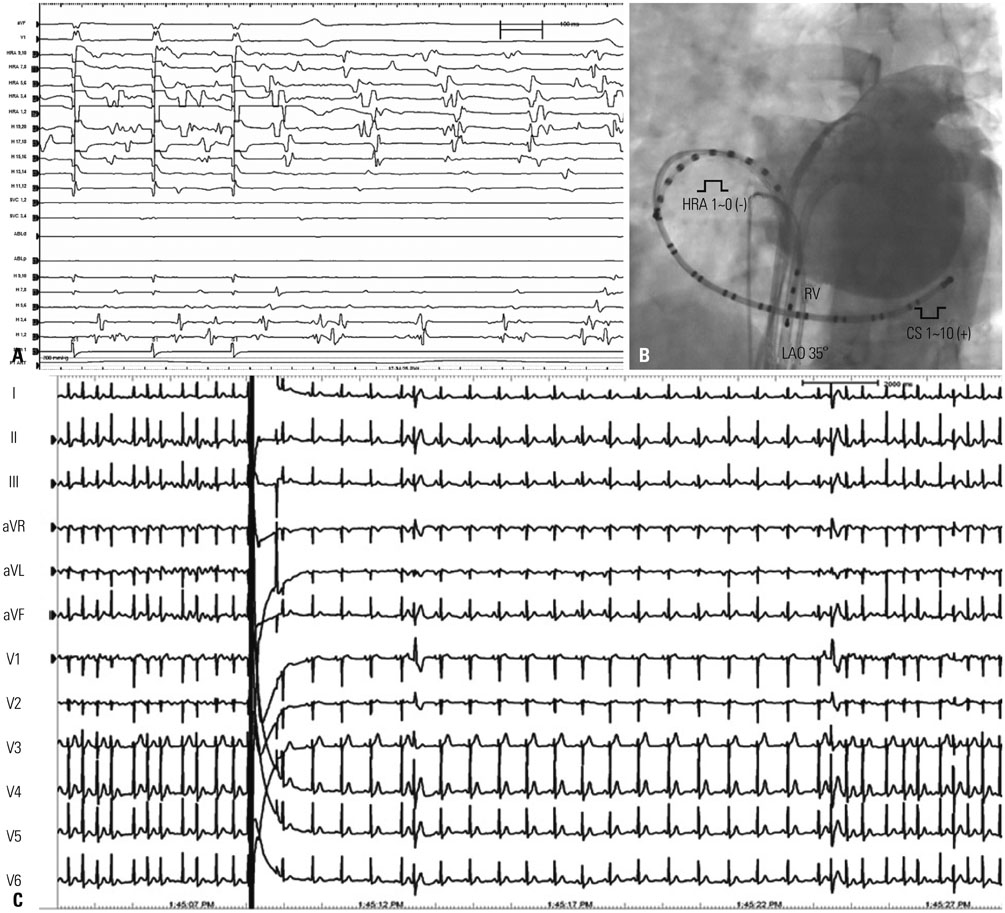
Fig. 2 (A) Inducibility test by high-current HRA pacing for 10 sec. AF or AT maintenance longer than 3 min was considered positive inducibility. (B) Catheter position for mapping and cardioversion. For the IRAPB test, we delivered internal cardioversion shock from HRA to CS. (C) An example of IRAPB after cardioversion under isoproterenol infusion. CS, coronary sinus; HRA, high right atrium; LAO, left anterior oblique view; RV, right ventricle; AF, atrial fibrillation; AT, atrial tachycardia; IRAPB, immediate recurrence of atrial premature beat.
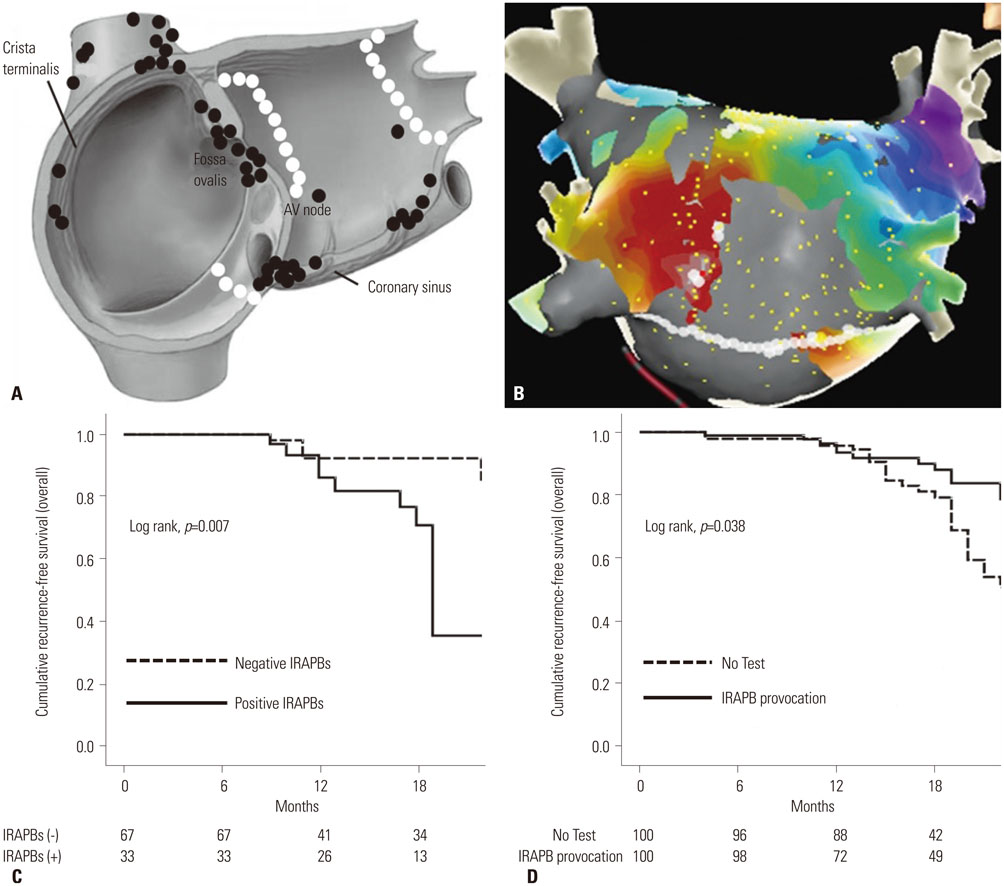
Fig. 3 (A) Locations of post-procedural IRAPBs and additional ablation sites (black circles). White circles indicate the standard ablation sites for PAF. (B)Mapping and ablation of post-procedural IRAPB utilizing 3D activation map. Quick activation mapping by multipolar catheter revealed non-PV foci located on LA posterior wall (white dots) and conduction gap at posterior inferior linear ablation site. We eliminated IRAPBs and ablation gap on posterior inferior line concomitantly. (C) Kaplan-Meier curve for AF-free survival comparing patients with post-procedural IRAPBs to those without IRAPBs. (D) Kaplan-Meier graph of AF-free survival comparing the IRAPB provocation group to the No-Test group. IRAPBs, immediate recurrence of atrial premature beats; 3D, three-dimensional; PV, pulmonary vein; LA, left atrial; AF, atrial fibrillation; PAF, paroxysmal AF.
Cited by 1 articles
-
Unilateral versus Bilateral Groin Puncture for Atrial Fibrillation Ablation: Multi-Center Prospective Randomized Study
Hee Tae Yu, Dong Geum Shin, Jaemin Shim, Gi-Byoung Nam, Won Woo Yoo, Ji Hyun Lee, Tae-Hoon Kim, Jae-Sun Uhm, Boyoung Joung, Moon-Hyoung Lee, Young-Hoon Kim, Hui-Nam Pak
Yonsei Med J. 2019;60(4):360-367. doi: 10.3349/ymj.2019.60.4.360.
Reference
-
1. Inoue K, Kurotobi T, Kimura R, Toyoshima Y, Itoh N, Masuda M, et al. Trigger-based mechanism of the persistence of atrial fibrillation and its impact on the efficacy of catheter ablation. Circ Arrhythm Electrophysiol. 2012; 5:295–301.
Article2. Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012; 33:2719–2747.3. European Heart Rhythm Association. European Association for Cardio-Thoracic Surgery. Camm AJ, Kirchhof P, Lip GY, Schotten U, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010; 31:2369–2429.4. Pak HN, Hwang C, Lim HE, Kim JW, Lee HS, Kim YH. Electroanatomic characteristics of atrial premature beats triggering atrial fibrillation in patients with persistent versus paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2006; 17:818–824.
Article5. Lee SH, Tai CT, Hsieh MH, Tsao HM, Lin YJ, Chang SL, et al. Predictors of non-pulmonary vein ectopic beats initiating paroxysmal atrial fibrillation: implication for catheter ablation. J Am Coll Cardiol. 2005; 46:1054–1059.
Article6. Oral H, Crawford T, Frederick M, Gadeela N, Wimmer A, Dey S, et al. Inducibility of paroxysmal atrial fibrillation by isoproterenol and its relation to the mode of onset of atrial fibrillation. J Cardiovasc Electrophysiol. 2008; 19:466–470.
Article7. Oral H, Chugh A, Good E, Sankaran S, Reich SS, Igic P, et al. A tailored approach to catheter ablation of paroxysmal atrial fibrillation. Circulation. 2006; 113:1824–1831.
Article8. Oral H, Chugh A, Lemola K, Cheung P, Hall B, Good E, et al. Noninducibility of atrial fibrillation as an end point of left atrial circumferential ablation for paroxysmal atrial fibrillation: a randomized study. Circulation. 2004; 110:2797–2801.
Article9. Gaita F, Caponi D, Pianelli M, Scaglione M, Toso E, Cesarani F, et al. Radiofrequency catheter ablation of atrial fibrillation: a cause of silent thromboembolism? Magnetic resonance imaging assessment of cerebral thromboembolism in patients undergoing ablation of atrial fibrillation. Circulation. 2010; 122:1667–1673.
Article10. Pak HN, Oh YS, Lim HE, Kim YH, Hwang C. Comparison of voltage map-guided left atrial anterior wall ablation versus left lateral mitral isthmus ablation in patients with persistent atrial fibrillation. Heart Rhythm. 2011; 8:199–206.
Article11. Hwang ES, Nam GB, Joung B, Park J, Lee JS, Shim J, et al. Significant reduction of atrial defibrillation threshold and inducibility by catheter ablation of atrial fibrillation. Pacing Clin Electrophysiol. 2012; 35:1428–1435.
Article12. Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, et al. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010; 3:32–38.
Article13. European Heart Rhythm Association (EHRA). European Cardiac Arrhythmia Scoiety (ECAS). American College of Cardiology (ACC). American Heart Association (AHA). Society of Thoracic Surgeons (STS). Calkins H, et al. HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2007. 4:p. 816–861.
Article14. Wazni O, Wilkoff B, Saliba W. Catheter ablation for atrial fibrillation. N Engl J Med. 2011; 365:2296–2304.
Article15. Coumel P. Paroxysmal atrial fibrillation: a disorder of autonomic tone? Eur Heart J. 1994; 15:Suppl A. 9–16.
Article16. Coumel P. Autonomic influences in atrial tachyarrhythmias. J Cardiovasc Electrophysiol. 1996; 7:999–1007.
Article17. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998; 339:659–666.
Article18. Pappone C, Rosanio S, Oreto G, Tocchi M, Gugliotta F, Vicedomini G, et al. Circumferential radiofrequency ablation of pulmonary vein ostia: a new anatomic approach for curing atrial fibrillation. Circulation. 2000; 102:2619–2628.
Article19. Kumar S, Kalman JM, Sutherland F, Spence SJ, Finch S, Sparks PB. Atrial fibrillation inducibility in the absence of structural heart disease or clinical atrial fibrillation: critical dependence on induction protocol, inducibility definition, and number of inductions. Circ Arrhythm Electrophysiol. 2012; 5:531–536.
Article20. Chen SA, Hsieh MH, Tai CT, Tsai CF, Prakash VS, Yu WC, et al. Initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins: electrophysiological characteristics, pharmacological responses, and effects of radiofrequency ablation. Circulation. 1999; 100:1879–1886.
Article21. Pappone C, Santinelli V, Manguso F, Vicedomini G, Gugliotta F, Augello G, et al. Pulmonary vein denervation enhances long-term benefit after circumferential ablation for paroxysmal atrial fibrillation. Circulation. 2004; 109:327–334.
Article22. Krul SP, Driessen AH, van Boven WJ, Linnenbank AC, Geuzebroek GS, Jackman WM, et al. Thoracoscopic video-assisted pulmonary vein antrum isolation, ganglionated plexus ablation, and periprocedural confirmation of ablation lesions: first results of a hybrid surgical-electrophysiological approach for atrial fibrillation. Circ Arrhythm Electrophysiol. 2011; 4:262–270.
Article23. Edgerton JR, Brinkman WT, Weaver T, Prince SL, Culica D, Herbert MA, et al. Pulmonary vein isolation and autonomic denervation for the management of paroxysmal atrial fibrillation by a minimally invasive surgical approach. J Thorac Cardiovasc Surg. 2010; 140:823–828.
Article24. Oh S, Zhang Y, Bibevski S, Marrouche NF, Natale A, Mazgalev TN. Vagal denervation and atrial fibrillation inducibility: epicardial fat pad ablation does not have long-term effects. Heart Rhythm. 2006; 3:701–708.
Article25. Schauerte P, Scherlag BJ, Pitha J, Scherlag MA, Reynolds D, Lazzara R, et al. Catheter ablation of cardiac autonomic nerves for prevention of vagal atrial fibrillation. Circulation. 2000; 102:2774–2780.
Article26. Haissaguerre M, Hocini M, Shah AJ, Derval N, Sacher F, Jais P, et al. Noninvasive panoramic mapping of human atrial fibrillation mechanisms: a feasibility report. J Cardiovasc Electrophysiol. 2013; 24:711–717.
Article27. Haïssaguerre M, Hocini M, Sanders P, Sacher F, Rotter M, Takahashi Y, et al. Catheter ablation of long-lasting persistent atrial fibrillation: clinical outcome and mechanisms of subsequent arrhythmias. J Cardiovasc Electrophysiol. 2005; 16:1138–1147.
Article28. Konings KT, Smeets JL, Penn OC, Wellens HJ, Allessie MA. Configuration of unipolar atrial electrograms during electrically induced atrial fibrillation in humans. Circulation. 1997; 95:1231–1241.
Article29. Lo LW, Lin YJ, Tsao HM, Chang SL, Hu YF, Tsai WC, et al. Characteristics of complex fractionated electrograms in nonpulmonary vein ectopy initiating atrial fibrillation/atrial tachycardia. J Cardiovasc Electrophysiol. 2009; 20:1305–1312.
Article30. Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004; 43:2044–2053.
Article31. Verma A, Mantovan R, Macle L, De Martino G, Chen J, Morillo CA, et al. Substrate and Trigger Ablation for Reduction of Atrial Fibrillation (STAR AF): a randomized, multicentre, international trial. Eur Heart J. 2010; 31:1344–1356.
Article32. Lemery R, Birnie D, Tang AS, Green M, Gollob M. Feasibility study of endocardial mapping of ganglionated plexuses during catheter ablation of atrial fibrillation. Heart Rhythm. 2006; 3:387–396.
Article33. Shim J, Joung B, Park JH, Uhm JS, Lee MH, Pak HN. Long duration of radiofrequency energy delivery is an independent predictor of clinical recurrence after catheter ablation of atrial fibrillation: over 500 cases experience. Int J Cardiol. 2013; 167:2667–2672.
Article34. Kim JB, Yang DH, Kang JW, Jung SH, Choo SJ, Chung CH, et al. Left atrial function following surgical ablation of atrial fibrillation: prospective evaluation using dual-source cardiac computed tomography. Yonsei Med J. 2015; 56:608–616.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- Large Circular Ring Catheter Ablation Versus Anatomically Guided Ablation of Atrial Fibrillation: Back to the Future for Successful Catheter Ablation of Atrial Fibrillation?
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
