Airway management of a patient incidentally diagnosed with Mounier-Kuhn syndrome during general anesthesia
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul, Republic of Korea. jungman007@gmail.com
- 2Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Republic of Korea.
- 3Department of Anesthesiology and Pain Medicine, Seoul National University Hospital, Seoul, Republic of Korea.
- KMID: 2461247
- DOI: http://doi.org/10.17245/jdapm.2019.19.5.301
Abstract
- Mounier-Kuhn syndrome (MKS) is a disease characterized by dilation of the trachea and mainstem bronchi. Due to the risk of airway leakage, pulmonary aspiration, and tracheal damage, MKS can be fatal in patients undergoing tracheal intubation. Moreover, MKS may not be diagnosed preoperatively due to its rarity. In this case, a patient undergoing neurosurgery was incidentally diagnosed with MKS during general anesthesia. During anesthesia induction, difficulties in airway management led the anesthesiologist to suspect MKS. Airway leakage was resolved in this case using oropharyngeal gauze packing. Anesthesiologists should be aware of the possibility of MKS and appropriate management of the airways.
MeSH Terms
Figure
-
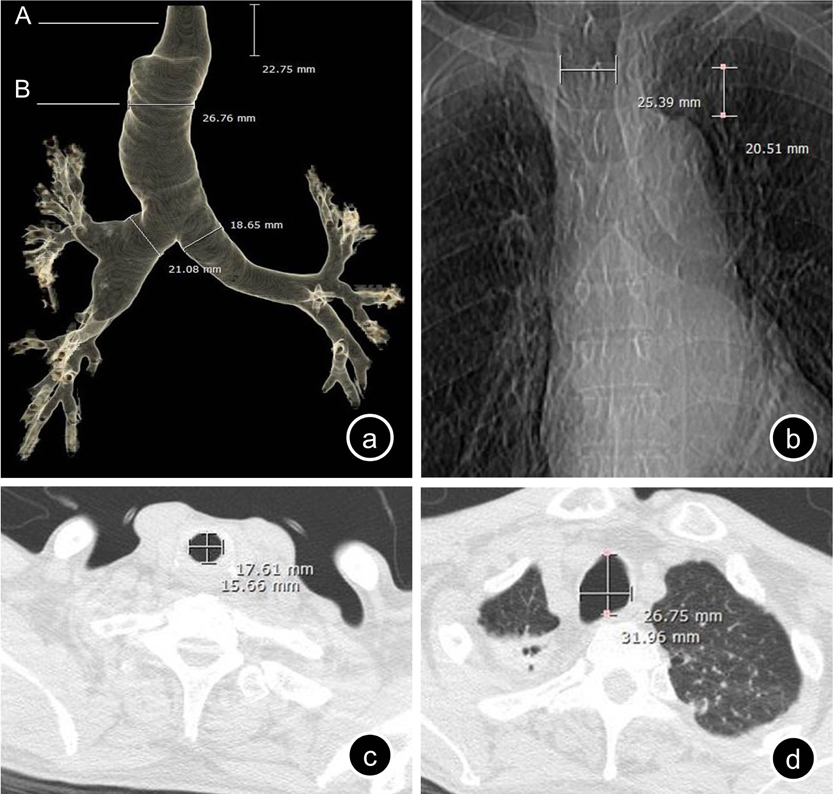
Fig. 1 (a) Anteroposterior view of the three-dimensional reconstruction of the thoracic computed tomography (CT) images. There is a relatively un-dilated area of the trachea in the subglottic region of approximately 2 cm in length. (b) Scanogram of preoperative chest CT clearly shows dilation of the trachea. (c) Axial plane of the thoracic CT at point ‘A’ in (a) showing relatively normal tracheal diameter. (d) Axial plane of the thoracic CT at point ‘B’ in (a) showing dilation of the trachea 2 cm above the aortic arch.
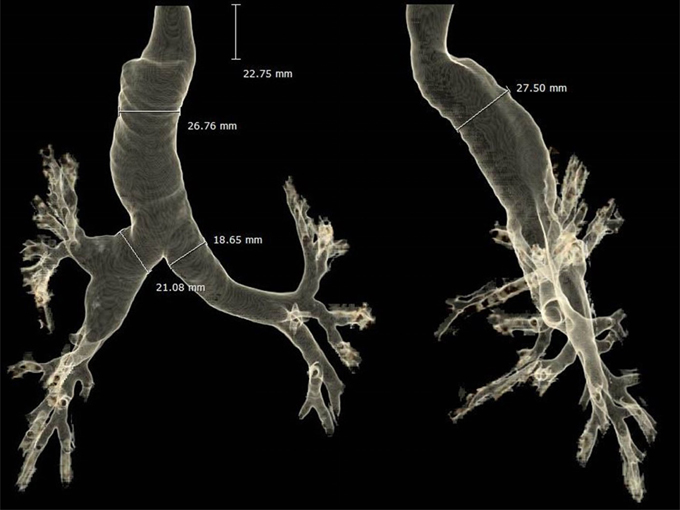
Fig. 2 Three-dimensional reconstruction of the preoperative thoracic computed tomography images showing severe dilation of the trachea and mainstem bronchi. Anteroposterior (left) and lateral (right) views.
Cited by 1 articles
-
Airway management of a patient with Mounier-Kuhn syndrome during general anesthesia - A case report -
Boreum Cheon, Ju Hyung Lee, Jae Hyung Kim, Sung Mi Hwang
Anesth Pain Med. 2024;19(2):156-160. doi: 10.17085/apm.23172.
Reference
-
1. Krustins E. Mounier-kuhn syndrome: A systematic analysis of 128 cases published within last 25 years. Clin Respir J. 2016; 10:3–10.
Article2. Min JJ, Lee JM, Kim JH, Hong DM, Jeon Y, Bahk JH. Anesthetic management of a patient with Mounier-Kuhn syndrome undergoing off-pump coronary artery bypass graft surgery -A case report-. Korean J Anesthesiol. 2011; 61:83–87.
Article3. Breatnach E, Abbott GC, Fraser RG. Dimensions of the normal human trachea. AJR Am J Roentgenol. 1984; 142:903–906.
Article4. Katz I, Levine M, Herman P. Tracheobronchiomegaly. The Mounier-Kuhn syndrome. Am J Roentgenol Radium Ther Nucl Med. 1962; 88:1084–1094.5. Vock P, Spiegel T, Fram EK, Effmann EL. CT assessment of the adult intrathoracic cross section of the trachea. J Comput Assist Tomogr. 1984; 8:1076–1082.
Article6. Van Schoor J, Joos G, Pauwels R. Tracheobronchomegaly--the mounier-kuhn syndrome: Report of two cases and review of the literature. Eur Respir J. 1991; 4:1303–1306.7. Bourne TM, Raphael JH, Tordoff SG. Anaesthesia for a patient with tracheobronchomegaly (mounier-kuhn syndrome). Anaesthesia. 1995; 50:545–546.
Article8. Maxwell MJ, Pollock JG, Iftikhar SY, Chesshire NJ. One-lung ventilation in a patient with tracheobronchomegaly: A case report and literature review. Eur J Anaesthesiol. 2009; 26:797–799.
Article9. Imashuku Y, Kitagawa H, Fukushima Y, Aoi R. Anesthesia with the proseal laryngeal mask airway for a patient with mounier-kuhn syndrome. J Clin Anesth. 2010; 22:154.
Article10. Ushakumari DS, Grewal N, Green M. Mounier-kuhn syndrome: Anesthetic experience. Case Rep Anesthesiol. 2012; 2012:674918.
Article11. Cataldo R, Galli B, Proscia P, Carassiti M. Management of a patient with Mounier-Kuhn syndrome undergoing repeated general anesthetics. Can J Anaesth. 2013; 60:602–603.
Article12. Subramani S, Freeman B, Rajagopal S. Anesthetic considerations for bilateral lung transplantation in mounier-kuhn syndrome. J Cardiothorac Vasc Anesth. 2015; 29:727–730.
Article13. Woodring JH, Barrett PA, Rehm SR, Nurenberg P. Acquired tracheomegaly in adults as a complication of diffuse pulmonary fibrosis. AJR Am J Roentgenol. 1989; 152:743–747.
Article14. Messahel FM. Tracheal dilatation followed by stenosis in mounier-kuhn syndrome. A case report. Anaesthesia. 1989; 44:227–229.
Article15. Mondoni M, Carlucci P, Parazzini EM, Busatto P, Centanni S. Huge tracheal diverticulum in a patient with mounierkuhn syndrome. Eur J Case Rep Intern Med. 2016; 3:000419.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Airway management of a patient with Mounier-Kuhn syndrome during general anesthesia - A case report -
- Anesthetic management of a patient with Mounier-Kuhn syndrome undergoing off-pump coronary artery bypass graft surgery: A case report
- A Case Report of Lung Cancer with Tracheobronchomegaly: A Case Report of Mounier: Kuhn syndrome
- A Case of Tracheobronchomegaly with Pneumonia
- Perioperative airway management of a patient with Beckwith-Wiedemann syndrome
