Embolotherapy of Ruptured Gastroepiploico-Colic Communicating Artery with Median Arcuate Ligament Syndrome: A Case Report
- Affiliations
-
- 1Department of Radiology, Myongji Hospital, Hanyang University College of Medicine, Goyang, Korea. parkjh4803@gmail.com
- KMID: 2459021
- DOI: http://doi.org/10.3348/jksr.2019.80.5.958
Abstract
- Aneurysm of collateral vessels in celiac axis stenosis has seldom been reported. We report a case of hemoperitoneum due to spontaneous aneurysmal rupture of a previously unreported collateral vessel in a patient with median arcuate ligament syndrome. A 37-year-old man without any history of illness or trauma exhibited hemoperitoneum with an aneurysm in the right subhepatic area on CT. CT findings also included celiac stenosis due to median arcuate ligament thickening. Celiac and superior mesenteric artery angiography revealed an abnormal communicating artery aneurysm between the right gastroepiploic and right colic arteries. We named this aberrant anastomosis "gastroepiploico-colic communicating artery." This rare collateral channel may cause spontaneous aneurysmal rupture in the presence of celiac stenosis. We successfully treated the aneurysmal rupture by transcatheter arterial embolization.
MeSH Terms
Figure
-
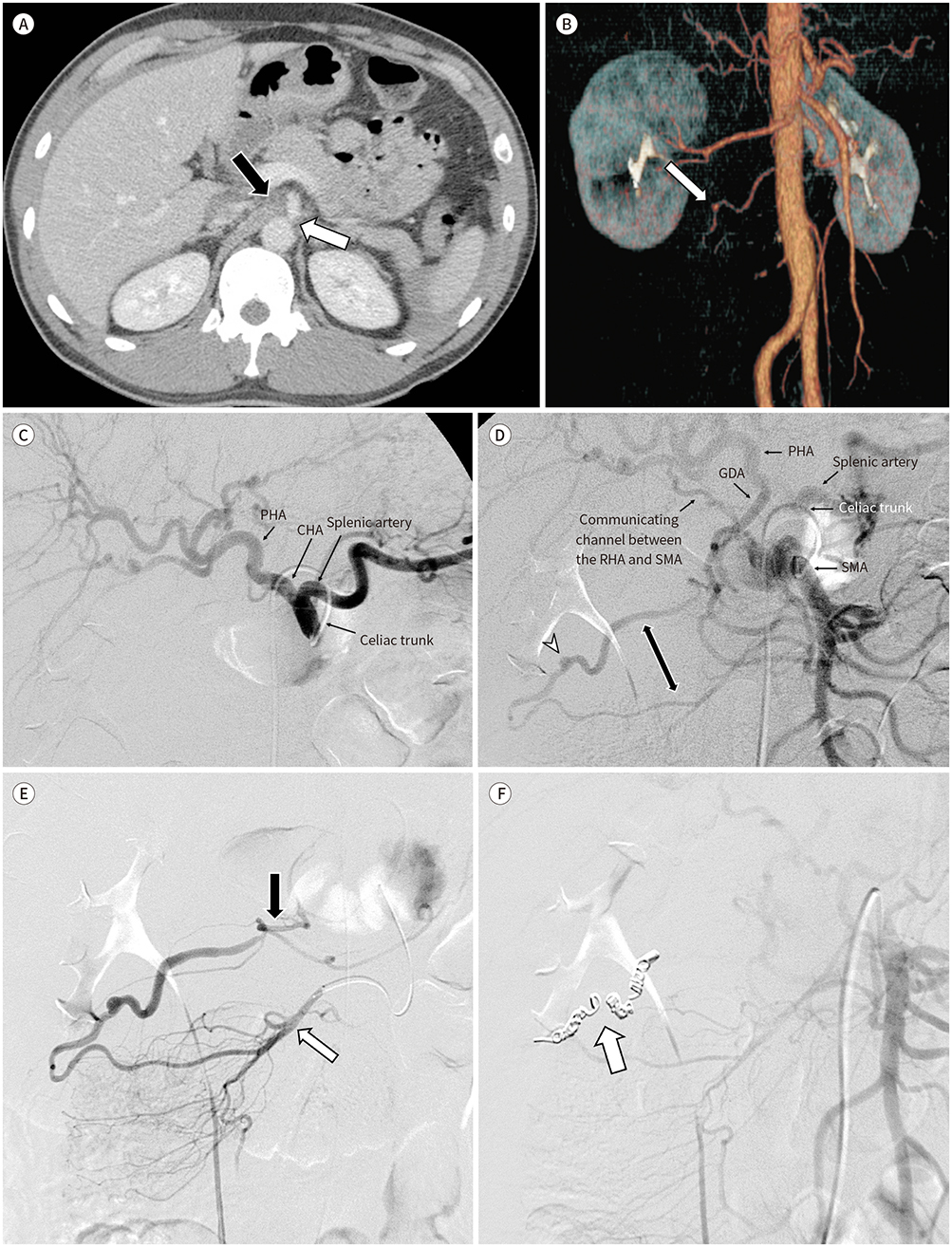
Fig. 1 Aneurysmal rupture of the aberrant collateral artery was treated by transcatheter arterial embolization. A. The median arcuate ligament (black arrow) appeared to be thickened and compressing the celiac trunk (white arrow), consistent with median arcuate ligament syndrome. B. Reconstructed CT angiography showed an aneurysm (arrow) in the right subhepatic area. C. The GDA was not visualized on celiac angiography. Only the CHA, PHA and splenic artery were visible (arrows). D. SMA angiography revealed opacification of the GDA, PHA, splenic artery and the communicating channels between the RHA and SMA (black arrows). The aneurysm (white arrowhead) in the “gastroepiploico-colic communicating artery” (two way arrow). E. The “gastroepiploico-colic communicating artery” between the right gastroepiploic artery (black arrow) and right colic artery (white arrow) on right colic arteriography. F. Embolization was performed at the distal and proximal portions of the aneurysm in the “gastroepiploico-colic communicating artery” with microcoils using a microcatheter (arrow). CHA = common hepatic artery, GDA = gastroduodenal artery, PHA = proper hepatic artery, RHA = right hepatic artery, SMA = superior mesenteric artery
Reference
-
1. Sakorafas GH, Sarr MG, Peros G. Celiac artery stenosis: an underappreciated and unpleasant surprise in patients undergoing pancreaticoduodenectomy. J Am Coll Surg. 2008; 206:349–356.
Article2. Antoniak R, Grabowska-Derlatka L, Nawrot I, Cieszanowski A, Rowiński O. Aneurysms of peripancreatic arterial arcades coexisting with celiac trunk stenosis or occlusion: single institution experience. Biomed Res Int. 2017; 2017:1645013.
Article3. Vandy FC, Sell KA, Eliason JL, Coleman DM, Rectenwald JE, Stanley JC. Pancreaticoduodenal and gastroduodenal artery aneurysms associated with celiac artery occlusive disease. Ann Vasc Surg. 2017; 41:32–40.
Article4. Ogino H, Sato Y, Banno T, Arakawa T, Hara M. Embolization in a patient with ruptured anterior inferior pancreaticoduodenal arterial aneurysm with median arcuate ligament syndrome. Cardiovasc Intervent Radiol. 2002; 25:318–319.
Article5. Nasr LA, Faraj WG, Al-Kutoubi A, Hamady M, Khalifeh M, Hallal A, et al. Median arcuate ligament syndrome: a single-center experience with 23 patients. Cardiovasc Intervent Radiol. 2017; 40:664–670.
Article6. Jesinger RA, Thoreson AA, Lamba R. Abdominal and pelvic aneurysms and pseudoaneurysms: imaging review with clinical, radiologic, and treatment correlation. Radiographics. 2013; 33:E71–E96.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic management of median arcuate ligament syndrome: a video vignette
- Open surgical decompression of celiac axis compression by division of the median arcuate ligament
- Clinical and Radiologic Review of Uncommon Cause of Profound Iron Deficiency Anemia: Median Arcuate Ligament Syndrome
- Celiac Axis Compression Syndrome
- Pancreaticoduodenal Artery Aneurysm due to Median Arcuate Ligament Compression of the Celiac Artery
