The PREVAIL trial of enzalutamide in men with chemotherapy-naïve, metastatic castration-resistant prostate cancer: Post hoc analysis of Korean patients
- Affiliations
-
- 1Department of Urology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. cskim@amc.seoul.kr
- 2Biostatistics, Astellas Pharma Europe B.V., Leiden, The Netherlands.
- 3Department of Urology, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Gwangju, Korea.
- 4Department of Urology, Severance Hospital, Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Urology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Urology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 7Department of Urology, Center for Prostate Cancer, National Cancer Center, Goyang, Korea.
- 8Department of Urology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2426491
- DOI: http://doi.org/10.4111/icu.2016.57.3.174
Abstract
- PURPOSE
This post hoc analysis evaluated treatment effects, safety, and pharmacokinetics of enzalutamide in Korean patients in the phase 3, double-blind, placebo-controlled PREVAIL trial.
MATERIALS AND METHODS
Asymptomatic or mildly symptomatic chemotherapy-naive men with metastatic castration-resistant prostate cancer that progressed on androgen deprivation therapy received 160 mg/d oral enzalutamide or placebo (1:1) until death or discontinuation due to radiographic progression or skeletal-related event and initiation of subsequent therapy. Coprimary end points were centrally assessed radiographic progression-free survival (rPFS) and overall survival (OS). Secondary end points included investigator-assessed rPFS, time to initiation of chemotherapy, time to prostate-specific antigen (PSA) progression, PSA response (≥50% decline), and time to skeletal-related event.
RESULTS
Of 1,717 total patients, 78 patients were enrolled in Korea (enzalutamide, n=40; placebo, n=38). Hazard ratios (95% confidence interval) for enzalutamide versus placebo were 0.23 (0.02-2.24) for centrally assessed rPFS, 0.77 (0.28-2.15) for OS, 0.21 (0.08-0.51) for time to chemotherapy, and 0.31 (0.17-0.56) for time to PSA progression. A PSA response was observed in 70.0% of enzalutamide-treated and 10.5% of placebo-treated Korean patients. Adverse events of grade ≥3 occurred in 33% of enzalutamide-treated and 11% of placebo-treated Korean patients, with median treatment durations of 13.0 and 5.1 months, respectively. At 13 weeks, the plasma concentration of enzalutamide plus N-desmethyl enzalutamide was similar in Korean and non-Korean patients (geometric mean ratio, 1.04; 90% confidence interval, 0.97-1.10).
CONCLUSIONS
In Korean patients, treatment effects and safety of enzalutamide were consistent with those observed in the overall PREVAIL study population (ClinicalTrials.gov Identifier: NCT01212991).
Keyword
MeSH Terms
-
Adenocarcinoma/blood/diagnostic imaging/drug therapy/*secondary
Administration, Oral
Adult
Aged
Aged, 80 and over
Antineoplastic Agents, Hormonal/adverse effects/blood/*therapeutic use
Antineoplastic Combined Chemotherapy Protocols/therapeutic use
Disease Progression
Double-Blind Method
Humans
Kallikreins/blood
Male
Middle Aged
Phenylthiohydantoin/adverse effects/*analogs & derivatives/blood/therapeutic use
Prostate-Specific Antigen/blood
Prostatic Neoplasms, Castration-Resistant/blood/diagnostic imaging/*drug therapy
Radiography
Survival Analysis
Treatment Outcome
Antineoplastic Agents, Hormonal
Phenylthiohydantoin
Kallikreins
Prostate-Specific Antigen
Figure
-
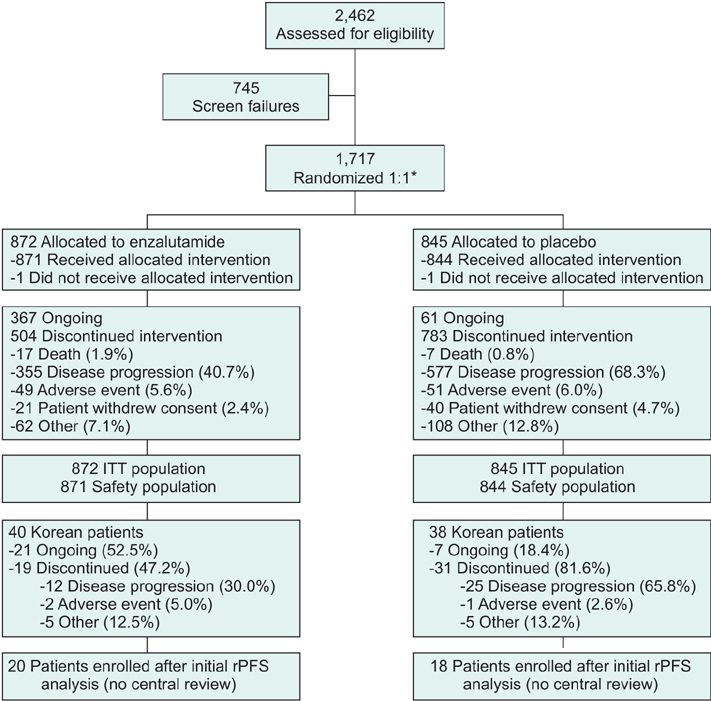
Fig. 1 PREVAIL patient disposition. ITT, intent-to-treat; rPFS, radiographic progression-free survival. *Randomization was stratified by study site.
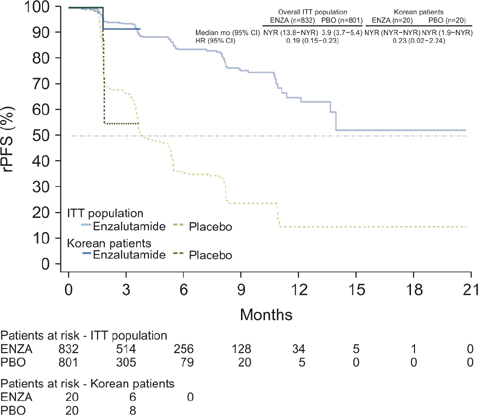
Fig. 2 Duration of centrally assessed rPFS in Korean patients and the overall study population (data cutoff May 6, 2012). Dashed horizontal line indicates median. Hazard ratios are based on unstratified Cox regression models with treatment as the only covariate and values <1.00 favoring enzalutamide. CI, confidence interval; ENZA, enzalutamide; HR, hazard ratio; ITT, intent-to-treat; NYR, not yet reached; PBO, placebo; rPFS, radiographic progression-free survival.
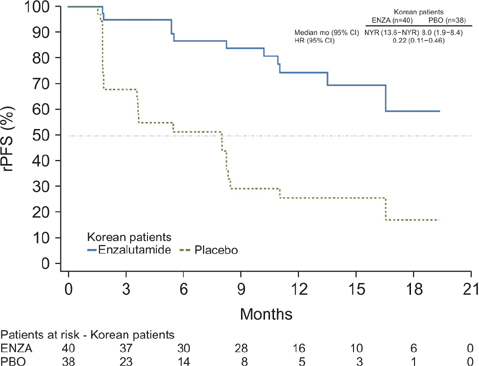
Fig. 3 Duration of investigator-assessed rPFS in Korean patients (data cutoff September 16, 2013). Dashed horizontal line indicates median. Hazard ratios are based on unstratified Cox regression models with treatment as the only covariate and values <1.00 favoring enzalutamide. CI, confidence interval; ENZA, enzalutamide; HR, hazard ratio; ITT, intent-to-treat; NYR, not yet reached; PBO, placebo; rPFS, radiographic progression-free survival.
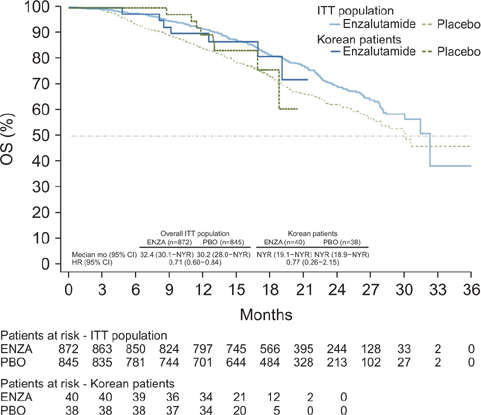
Fig. 4 Duration of OS in Korean patients and the overall study population (data cutoff Sep 16, 2013). Dashed horizontal line indicates median. Hazard ratios are based on unstratified Cox regression models with treatment as the only covariate and values <1.00 favoring enzalutamide. CI, confidence interval; ENZA, enzalutamide; HR, hazard ratio; ITT, intent-to-treat; NYR, not yet reached; OS, overall survival; PBO, placebo.
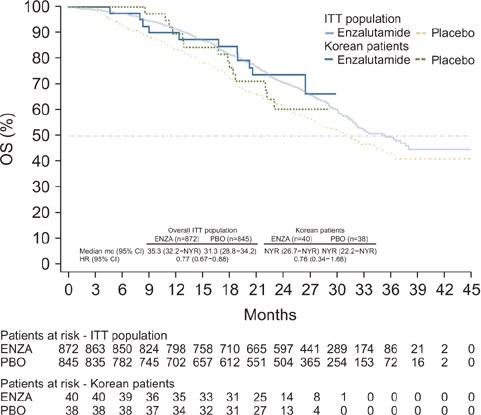
Fig. 5 Updated analysis of OS in Korean patients (data cutoff June 1, 2014). Dashed horizontal line indicates median. Hazard ratios are based on unstratified Cox regression models with treatment as the only covariate and values <1.00 favoring enzalutamide. CI, confidence interval; ENZA, enzalutamide; HR, hazard ratio; ITT, intent-to-treat; NYR, not yet reached; OS, overall survival; PBO, placebo.
Cited by 2 articles
-
Enzalutamide in chemotherapy-naive patients with metastatic castration-resistant prostate cancer: A retrospective Korean multicenter study in a real-world setting
Seung Il Jung, Myung Soo Kim, Chang Wook Jeong, Cheol Kwak, Sung Kyu Hong, Seok Ho Kang, Jae Young Joung, Seung Hwan Lee, Seok Joong Yun, Tae-Hwan Kim, Sung Woo Park, Seong Soo Jeon, Minyong Kang, Ji Youl Lee, Byung Ha Chung, Jun Hyuk Hong, Hanjong Ahn, Choung-Soo Kim, Dong Deuk Kwon
Investig Clin Urol. 2020;61(1):19-27. doi: 10.4111/icu.2020.61.1.19.Oncological Outcomes in Men with Metastatic Castration-Resistant Prostate Cancer Treated with Enzalutamide with versus without Confirmatory Bone Scan
Chang Wook Jeong, Jang Hee Han, Dong Deuk Kwon, Jae Young Joung, Choung-Soo Kim, Hanjong Ahn, Jun Hyuk Hong, Tae-Hwan Kim, Byung Ha Chung, Seong Soo Jeon, Minyong Kang, Sung Kyu Hong, Tae Young Jung, Sung Woo Park, Seok Joong Yun, Ji Yeol Lee, Seung Hwan Lee, Seok Ho Kang, Cheol Kwak
Cancer Res Treat. 2024;56(2):634-641. doi: 10.4143/crt.2023.848.
Reference
-
1. Jung KW, Won YJ, Kong HJ, Oh CM, Cho H, Lee DH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2012. Cancer Res Treat. 2015; 47:127–141.2. Ferlay J, Soerjomataram I, Erik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 2013 [Internet]. Lyon (FR): International Agency for Research on Cancer;c2016. cited 2016 Jan 27. Available from: http://globocan.iarc.fr.3. Haas GP, Delongchamps N, Brawley OW, Wang CY, de la Roza G. The worldwide epidemiology of prostate cancer: perspectives from autopsy studies. Can J Urol. 2008; 15:3866–3871.4. Ito K. Prostate cancer in Asian men. Nat Rev Urol. 2014; 11:197–212.5. Lee DH, Jung HB, Chung MS, Lee SH, Chung BH. The change of prostate cancer treatment in Korea: 5 year analysis of a single institution. Yonsei Med J. 2013; 54:87–91.6. Curado MP, Edwards B, Shin HR, Storm H, Ferlay J, Heanue M, et al. Cancer Incidence in Five Continents, Vol. IX. IARC Scientific Publications No. 160; 2007 [Internet]. Lyon (FR): International Agency for Research on Cancer;c2016. cited 2016 Mar 20. Available from: http://www.iarc.fr/en/publications/pdfs-online/epi/sp160/.7. Forman D, Bray F, Brewster D, GombeMbalawa C, Kohler B, Pineros M, et al. Cancer incidence in five continents, Vol. X. IARC Scientific Publications No. 164; 2014 [Internet]. Lyon (FR): International Agency for Research on Cancer;c2016. cited 2016 Mar 20. Available from: http://ci5.iarc.fr/Default.aspx.8. Kirby M, Hirst C, Crawford ED. Characterising the castration-resistant prostate cancer population: a systematic review. Int J Clin Pract. 2011; 65:1180–1192.9. Feldman BJ, Feldman D. The development of androgen-independent prostate cancer. Nat Rev Cancer. 2001; 1:34–45.10. Pienta KJ, Bradley D. Mechanisms underlying the development of androgen-independent prostate cancer. Clin Cancer Res. 2006; 12:1665–1671.11. Scher HI, Sawyers CL. Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. J Clin Oncol. 2005; 23:8253–8261.12. Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008; 26:1148–1159.13. Berthold DR, Pond GR, Soban F, de Wit R, Eisenberger M, Tannock IF. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 study. J Clin Oncol. 2008; 26:242–245.14. Tannock IF, de Wit R, Berry WR, Horti J, Pluzanska A, Chi KN, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004; 351:1502–1512.15. Seruga B, Ocana A, Tannock IF. Drug resistance in metastatic castration-resistant prostate cancer. Nat Rev Clin Oncol. 2011; 8:12–23.16. Montgomery RB, Mostaghel EA, Vessella R, Hess DL, Kalhorn TF, Higano CS, et al. Maintenance of intratumoral androgens in metastatic prostate cancer: a mechanism for castration-resistant tumor growth. Cancer Res. 2008; 68:4447–4454.17. Chen CD, Welsbie DS, Tran C, Baek SH, Chen R, Vessella R, et al. Molecular determinants of resistance to antiandrogen therapy. Nat Med. 2004; 10:33–39.18. Knudsen KE, Scher HI. Starving the addiction: new opportunities for durable suppression of AR signaling in prostate cancer. Clin Cancer Res. 2009; 15:4792–4798.19. Tran C, Ouk S, Clegg NJ, Chen Y, Watson PA, Arora V, et al. Development of a second-generation antiandrogen for treatment of advanced prostate cancer. Science. 2009; 324:787–790.20. Beer TM, Armstrong AJ, Rathkopf DE, Loriot Y, Sternberg CN, Higano CS, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med. 2014; 371:424–433.21. Scher HI, Fizazi K, Saad F, Taplin ME, Sternberg CN, Miller K, et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012; 367:1187–1197.22. Saad F, de Bono J, Shore N, Fizazi K, Loriot Y, Hirmand M, et al. Efficacy outcomes by baseline prostate-specific antigen quartile in the AFFIRM trial. Eur Urol. 2015; 67:223–230.23. Loriot Y, Miller K, Sternberg CN, Fizazi K, De Bono JS, Chowdhury S, et al. Effect of enzalutamide on health-related quality of life, pain, and skeletal-related events in asymptomatic and minimally symptomatic, chemotherapy-naive patients with metastatic castration-resistant prostate cancer (PREVAIL): results from a randomised, phase 3 trial. Lancet Oncol. 2015; 16:509–521.24. Astellas Pharma Korea Inc.Xtandi [prescribing information]. Seoul: Astellas Pharma Korea Inc.;c2016. updated 2015 May 22. cited 2016 Mar 20. Available from: http://www.astellas.co.kr/product/pdf/xtand_150522.pdf.25. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994; 23:129–138.26. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. European Organization for Research and Treatment of Cancer. National Cancer Institute of the United States. National Cancer Institute of Canada. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000; 92:205–216.27. U.S. Department of Health and Human Services. U.S. Food and Drug Administration. Center for Drug Evaluation and Research. Center for Veterinary Medicine. Guidance for industry: bioanalytical method validation 2001 [Internet]. Silver Spring(MD): U.S. Food and Drug Administration;c2016. cited 2016 Jan 30. Available from: http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM070107.28. Oesterling JE, Kumamoto Y, Tsukamoto T, Girman CJ, Guess HA, Masumori N, et al. Serum prostate-specific antigen in a community-based population of healthy Japanese men: lower values than for similarly aged white men. Br J Urol. 1995; 75:347–353.29. Chia SE, Lau WK, Cheng C, Chin CM, Tan J, Ho SH. Prostate-specific antigen levels among Chinese, Malays and Indians in Singapore from a community-based study. Asian Pac J Cancer Prev. 2007; 8:375–378.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chemotherapy With Androgen Deprivation for Hormone-Naïve Prostate Cancer
- The Current Status of Metastatic Castration-Naïve Prostate Cancer Management
- Role of Androgen Receptor in Prostate Cancer: A Review
- Serum Testosterone Level as Possible Predictive Marker for Prognosis in Metastatic Castration-Resistant Prostate Cancer Patients Treated With Enzalutamide
- Systemic Therapies for Metastatic Castration-Resistant Prostate Cancer: An Updated Review
