Supplementary Diagnostic Landmarks of Left Ventricular Non-Compaction on Magnetic Resonance Imaging
- Affiliations
-
- 1Department of Cardiology, University Hospital “Thalassotherapia Opatija,†Medical Faculty University of Rijeka, Opatija, Croatia. marcoboban@yahoo.com
- 2Department of Internal Medicine, Medical Faculty “J.J. Strossmayer†University of Osijek, Osijek, Croatia.
- 3Department of Radiology, University Hospital “Thalassotherapia Opatija,†Opatija, Croatia.
- 4Department of Cardiology-Arrhythmology and Electrophysiology, University Hospital “Sestre Milosrdnice,†Zagreb, Croatia.
- KMID: 2418850
- DOI: http://doi.org/10.3349/ymj.2018.59.1.63
Abstract
- PURPOSE
Diagnostic criteria for left ventricular non-compaction (LVNC) are still a matter of dispute. The aim of our present study was to test the diagnostic value of two novel diagnostic cardiac magnetic resonance (CMR) parameters: proof of non-compact (NC) myocardium blood flow using T2 sequences and changes in geometry of the left ventricle.
MATERIALS AND METHODS
The study included cases with LVNC and controls, from a data base formed in a period of 3.5 years (n=1890 exams), in which CMR protocol included T2 sequences. Measurement of perpendicular maximal and minimal end diastolic dimensions in the region with NC myocardium from short axis plane was recorded, and calculated as a ratio (MaxMinEDDR), while flow through trabecula was proven by intracavital T2-weighted hyperintensity (ICT2HI). LVNC diagnosis met the following three criteria: thickening of compact (C) layer, NC:C>2.3:1 and NC>20%LV.
RESULTS
The study included 200 patients; 71 with LVNC (35.5%; i.e., 3.76% of CMRs) and 129 (64.5%) controls. MaxMinEDDR in patients with LVNC was significantly different from that in controls (1.17±0.08 vs. 1.06±0.04, respectively; p < 0.001). MaxMinEDDR >1.10 had sensitivity of 91.6% [95% confidence intervals (CI) 82.5-96.8], specificity of 85.3% (95% CI 78.0-90.0), and area under curve (AUC) 0.919 (95% CI 0.872-0.953; p < 0.001) for LVNC. Existence of ICT2HI had sensitivity of 100.0% (95% CI 94.9-100.0), specificity of 91.5% (95% CI 85.3-95.7), and AUC 0.957 (95% CI 0.919-0.981; p < 0.001) for LVNC.
CONCLUSION
Two additional diagnostic parameters for LVNC were identified in this study. ICT2HI and geometric eccentricity of the ventricle both had relatively high sensitivity and specificity for diagnosing LVNC.
Keyword
MeSH Terms
Figure
-
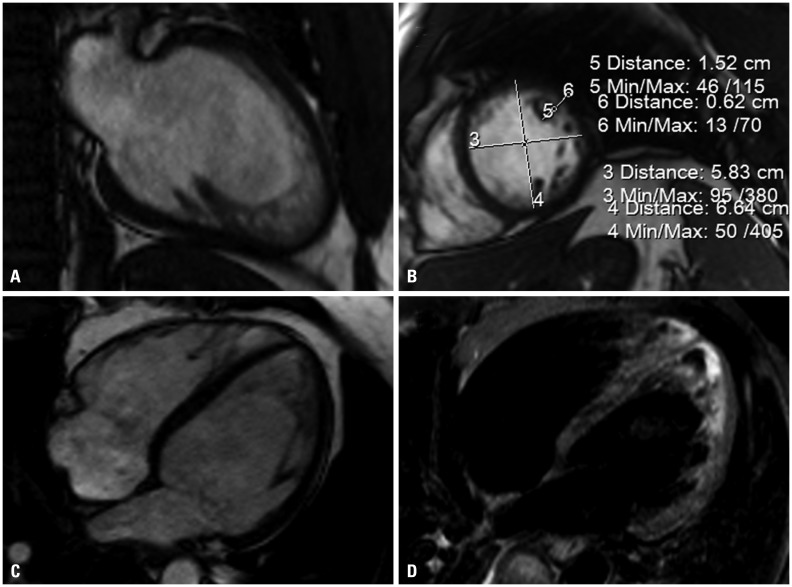
Fig. 1 Case of patient with LVNC. Case of LVNC with trabeculations existing on 23.5% of the left ventricle, left ventricle EDD of 6.29 cm, ejection fraction of 40% and confirmed non-compaction. (A) 2-chamber view, cine SSFP. (B) Short axis cine at end diastolic, marked white line showing: 3) Minimal EDD 5.83 cm, 4) Maximal EDD 6.64 cm, giving MaxMinEDDR=1.14; 5) NC-layer thickness 1.63 cm, and 6) C-layer thickness 0.42 cm, with NC:C=3.9; 4-chamber, cine SSFP. (C) 4-chamber, cine SSFP; showing trabeculations in apical region and lateral wall. (D) 4-chamber, turbo spin echo dark blood T2 fat saturation. Blood flow through non-compact layer is shown as hyperintense T2 signal, or the intracavital T-2 weighted hyperintensity, which is of high spontaneous contrast to the compact part of the myocardium and to endocavital space. LVNC, left ventricular non-compaction; EDD, end diastolic dimension; SSFP, steady state free precession.
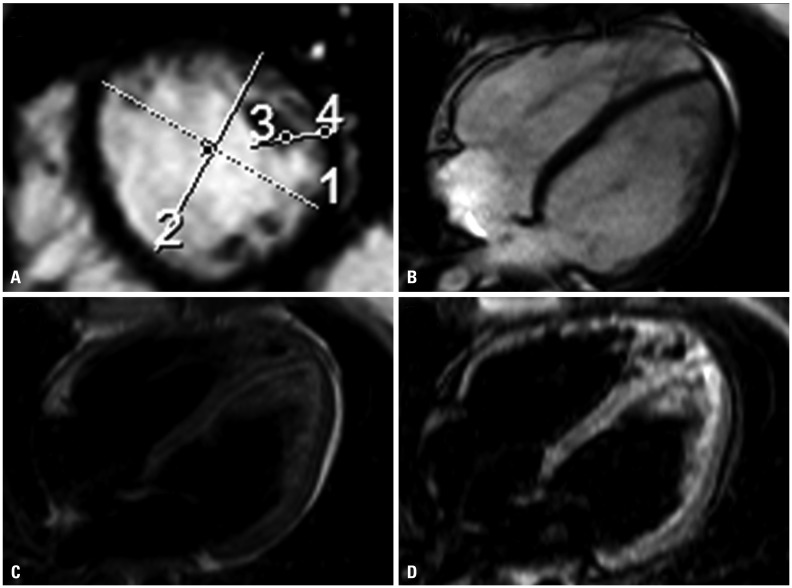
Fig. 2 Case two of LVNC. Case of LVNC with trabeculations existing on 23.5% of the left ventricle, ejection fraction of 50% and confirmed non-compaction. (A) short axis cine at end diastole, marked white line showing: 1) Maximal EDD 5.33 cm, 2) Minimal EDD 4.79 cm, giving MaxMinEDDR=1.11; 3) NC-layer thickness 1.63 cm, and 4) C-layer thickness 0.42 cm, with NC:C=3.9. (B) 4-chamber, cine steady state free precession, showing non-compact myocardium in apical and lateral wall. (C) 4-chamber turbo spin echo dark blood T2, showing intracavital hyperintense T2 signal. (D) 4-chamber, inversion recovery dark blood T2, showing intracavital hyperintense T2 signal. Blood flow through non-compact myocardium is shown as hyperintense T2 signal, i.e. ICT2HI, which is of high spontaneous contrast to the compact part of the myocardium and to endocavital space. ICT2HI, intracavital T2-weighted hyperintensity; MaxMinEDDR, maximal to minimal (perpendicular) end diastolic dimension ratio acquired in mid to apical short axis slices; NC:C, non-compact to compact myocardial layer thickness; NC>20%LV, percentage of trabeculations over 20% of total mass of the left ventricle. LVNC, left ventricular non-compaction; EDD, end diastolic dimension.
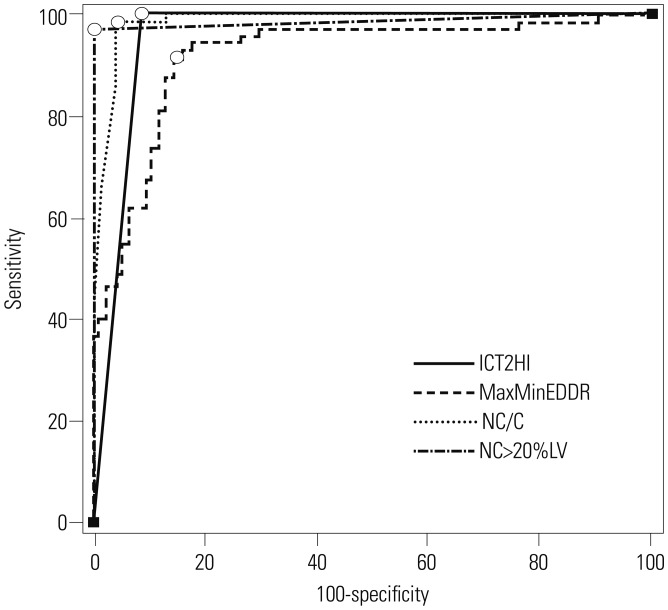
Fig. 3 Multiple receiver operating characteristic curve analysis for studied left ventricular non-compaction diagnostic parameters. ICT2HI, intracavital T-2 weighted hyperintensity; MaxMinEDDR, maximal to minimal end diastolic dimension ratio; NC/C, non-compact to compact myocardial layer thickness; NC<20%LV, percentage of trabeculations over 20% in total left ventricle mass. ◯ - ROC curve values with the highest Youden's Index.
Reference
-
1. Lofiego C, Biagini E, Pasquale F, Ferlito M, Rocchi G, Perugini E, et al. Wide spectrum of presentation and variable outcomes of isolated left ventricular non-compaction. Heart. 2007; 93:65–71. PMID: 16644854.
Article2. Bhatia NL, Tajik AJ, Wilansky S, Steidley DE, Mookadam F. Isolated noncompaction of the left ventricular myocardium in adults: a systematic overview. J Card Fail. 2011; 17:771–778. PMID: 21872148.
Article3. Oechslin EN, Attenhofer Jost CH, Rojas JR, Kaufmann PA, Jenni R. Long-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol. 2000; 36:493–500. PMID: 10933363.
Article4. Luxán G, Casanova JC, Martínez-Poveda B, Prados B, D’Amato G, MacGrogan D, et al. Mutations in the NOTCH pathway regulator MIB1 cause left ventricular noncompaction cardiomyopathy. Nat Med. 2013; 19:193–201. PMID: 23314057.
Article5. Olivotto I, d’Amati G, Basso C, Van Rossum A, Patten M, Emdin M, et al. Defining phenotypes and disease progression in sarcomeric cardiomyopathies: contemporary role of clinical investigations. Cardiovasc Res. 2015; 105:409–423. PMID: 25631583.
Article6. Xing Y, Ichida F, Matsuoka T, Isobe T, Ikemoto Y, Higaki T, et al. Genetic analysis in patients with left ventricular noncompaction and evidence for genetic heterogeneity. Mol Genet Metab. 2006; 88:71–77. PMID: 16427346.
Article7. Samsa LA, Yang B, Liu J. Embryonic cardiac chamber maturation: Trabeculation, conduction, and cardiomyocyte proliferation. Am J Med Genet C Semin Med Genet. 2013; 163C:157–168. PMID: 23720419.
Article8. Oechslin E, Jenni R. Left ventricular non-compaction revisited: a distinct phenotype with genetic heterogeneity? Eur Heart J. 2011; 32:1446–1456. PMID: 21285074.
Article9. Arbustini E, Weidemann F, Hall JL. Left ventricular noncompaction: a distinct cardiomyopathy or a trait shared by different cardiac diseases? J Am Coll Cardiol. 2014; 64:1840–1850. PMID: 25443708.10. Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, Anderson RH, et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol. 2005; 46:101–105. PMID: 15992642.11. Jenni R, Oechslin E, Schneider J, Attenhofer Jost C, Kaufmann PA. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001; 86:666–671. PMID: 11711464.
Article12. Grothoff M, Pachowsky M, Hoffmann J, Posch M, Klaassen S, Lehmkuhl L, et al. Value of cardiovascular MR in diagnosing left ventricular non-compaction cardiomyopathy and in discriminating between other cardiomyopathies. Eur Radiol. 2012; 22:2699–2709. PMID: 22772366.
Article13. Olivas-Chacon CI, Mullins C, Stewart K, Akle N, Calleros JE, Ramos-Duran LR. Magnetic resonance imaging of non-ischemic cardiomyopathies: a pictorial essay. J Clin Imaging Sci. 2015; 5:37. PMID: 26199786.
Article14. Marchal P, Lairez O, Cognet T, Chabbert V, Barrier P, Berry M, et al. Relationship between left ventricular sphericity and trabeculation indexes in patients with dilated cardiomyopathy: a cardiac magnetic resonance study. Eur Heart J Cardiovasc Imaging. 2013; 14:914–920. PMID: 23644933.
Article15. Lieb W, Gona P, Larson MG, Aragam J, Zile MR, Cheng S, et al. The natural history of left ventricular geometry in the community: clinical correlates and prognostic significance of change in LV geometric pattern. JACC Cardiovasc Imaging. 2014; 7:870–878. PMID: 25129518.16. Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008; 29:270–276. PMID: 17916581.
Article17. Jacquier A, Thuny F, Jop B, Giorgi R, Cohen F, Gaubert JY, et al. Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur Heart J. 2010; 31:1098–1104. PMID: 20089517.
Article18. Fazio G, Novo G, D’Angelo L, Visconti C, Sutera L, Grassedonio E, et al. Magnetic resonance in isolated noncompaction of the ventricular myocardium. Int J Cardiol. 2010; 140:367–369. PMID: 19111359.
Article19. Gati S, Chandra N, Bennett RL, Reed M, Kervio G, Panoulas VF, et al. Increased left ventricular trabeculation in highly trained athletes: do we need more stringent criteria for the diagnosis of left ventricular non-compaction in athletes? Heart. 2013; 99:401–408. PMID: 23393084.
Article20. Choudhary P, Hsu CJ, Grieve S, Smillie C, Singarayar S, Semsarian C, et al. Improving the diagnosis of LV non-compaction with cardiac magnetic resonance imaging. Int J Cardiol. 2015; 181:430–436. PMID: 25569272.
Article21. Stöllberger C, Finsterer J, Blazek G. Left ventricular hypertrabeculation/noncompaction and association with additional cardiac abnormalities and neuromuscular disorders. Am J Cardiol. 2002; 90:899–902. PMID: 12372586.
Article22. Partovi S, Fram EK, Karis JP. Fast spin echo MR imaging. Neuroimaging Clin N Am. 1999; 9:553–576. PMID: 10433645.23. Naganawa S, Jenner G, Cooper TG, Potchen EJ, Ishigaki T. Rapid MR imaging of the liver: comparison of twelve techniques for single breath-hold whole volume acquisition. Radiat Med. 1994; 12:255–261. PMID: 7724816.24. Pui MH, Chang SK. Comparison of inversion recovery fast spin-echo (FSE) with T2-weighted fat-saturated FSE and T1-weighted MR imaging in bone marrow lesion detection. Skeletal Radiol. 1996; 25:149–152. PMID: 8848745.
Article25. Kim HW, Van Assche L, Jennings RB, Wince WB, Jensen CJ, Rehwald WG, et al. Relationship of T2-weighted MRI myocardial hyperintensity and the ischemic area-at-risk. Circ Res. 2015; 117:254–265. PMID: 25972514.
Article26. Lurz P, Luecke C, Eitel I, Föhrenbach F, Frank C, Grothoff M, et al. Comprehensive cardiac magnetic resonance imaging in patients with suspected myocarditis: The MyoRacer-Trial. J Am Coll Cardiol. 2016; 67:1800–1811. PMID: 27081020.27. Yang Y, Safka K, Graham JJ, Roifman I, Zia MI, Wright GA, et al. Correlation of late gadolinium enhancement MRI and quantitative T2 measurement in cardiac sarcoidosis. J Magn Reson Imaging. 2014; 39:609–616. PMID: 23720077.
Article28. Allen BC, Mohammed TL, Tan CD, Miller DV, Williamson EE, Kirsch JS. Metastatic melanoma to the heart. Curr Probl Diagn Radiol. 2012; 41:159–164. PMID: 22818836.
Article29. Lachhab A, Doghmi N, Elfakir Y, Taoussi O, Benyass A, Haddour L, et al. Insights from magnetic resonance imaging of left ventricular non-compaction in adults of North African descent. Int Arch Med. 2012; 5:10. PMID: 22405292.
Article30. Choi Y, Kim SM, Lee SC, Chang SA, Jang SY, Choe YH. Quantification of left ventricular trabeculae using cardiovascular magnetic resonance for the diagnosis of left ventricular non-compaction: evaluation of trabecular volume and refined semi-quantitative criteria. J Cardiovasc Magn Reson. 2016; 18:24. PMID: 27142637.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Isolated Non-Compaction of the Left Ventricle in a Patient with New-Onset Heart Failure: Morphologic and Functional Evaluation with Cardiac Multidetector Computed Tomography
- Left Ventricular Non-compaction with Ventricular Aneurysms
- Magnetic Resonance Imaging of Transient Left Ventricular Apical Ballooning Related to Emotional Stress: a Case Report
- Isolated Left Ventricular Noncompaction with a Congenital Aneurysm Presenting with Recurrent Embolism
- Principles and Clinical Applications of Feature-Tracking Cardiac Magnetic Resonance Imaging: A Literature Review
