Risk Factors of Microscopic Invasion in Early Gastric Cancer
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea. ysksuh@gmail.com
- 2Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2398799
- DOI: http://doi.org/10.5230/jgc.2017.17.e37
Abstract
- PURPOSE
This study aimed to evaluate the clinical significance of microscopic invasion to determine the adequate resection margin in early gastric cancer (EGC).
MATERIALS AND METHODS
A retrospective review was performed that included patients who underwent gastrectomy for clinical early gastric cancer (cEGC) at Seoul National University Hospital between January 2007 and December 2010. After subtracting the microscopic resection margin from the gross resection margin for each proximal or distal resection margin, microscopic invasion was represented by the larger value. Microscopic invasion and its risk factors were analyzed according to the clinicopathologic characteristics.
RESULTS
In total, 861 patients were enrolled in the study. Microscopic invasion of cEGC was 6.0±12.8 mm, and the proportion of patients with microscopic invasion ≥0 mm was 78.4%. In the risk group, tumor location, pT stage, and differentiation did not significantly discriminate the presence of microscopic invasion. The microscopic invasion of EGC-IIb was 13.9±16.8 mm, which was significantly greater than that of EGC-I. No linear correlation was observed between the overall tumor size and microscopic invasion (R=0.030). The independent risk factors for microscopic invasion ≥20 mm were EGC-IIb vs. EGC-I/IIa/IIc/III (odds ratio [OR], 3.103; 95% confidence interval [CI], 1.533-6.282; P=0.002) and male vs. female sex (OR, 1.655; 95% CI, 1.012-2.705; P=0.045).
CONCLUSIONS
Male sex and EGC-IIb were independent risk factors for microscopic invasion ≥20 mm. Examination of intraoperative frozen sections is highly recommended to avoid resection margin involvement, especially in cases of EGC-IIb.
Keyword
MeSH Terms
Figure
-
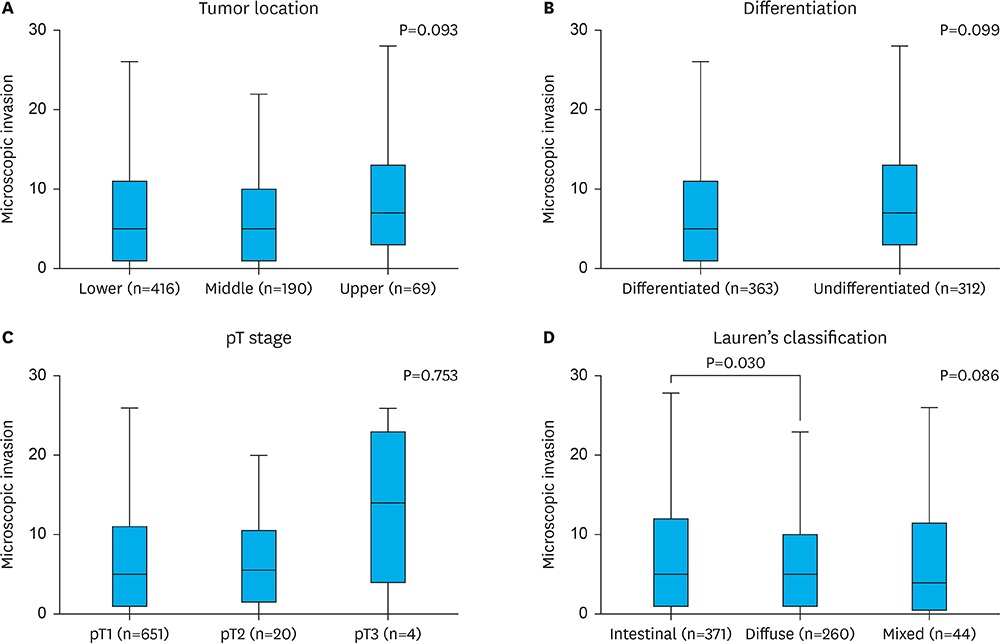
Fig. 1 Distribution of microscopic invasion according to the clinicopathologic characteristics in the risk group. Microscopic invasion according to (A) tumor location, (B) pT stage, (C) differentiation, and (D) Lauren's classification. Boxes indicate the interquartile ranges and median values; whiskers indicate the minimum and maximum values. P-values in the upper right corner were determined by Student's t-test or 1-way ANOVA. P-values in the upper section of the box (D) were generated using Student's t-test. ANOVA = analysis of variance.
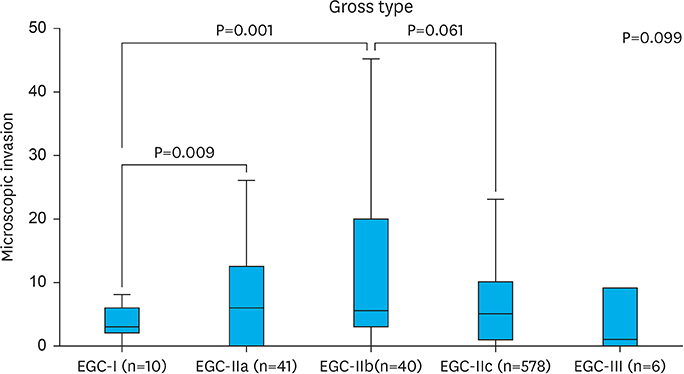
Fig. 2 Distribution of microscopic invasion according to gross type in the risk group. Boxes indicate the interquartile ranges and median values; whiskers indicate the minimum and maximum values. The P-value in the upper right corner was determined by 1-way ANOVA. P-values in the upper section of the box were generated using Student's t-test. ANOVA = analysis of variance; EGC = early gastric cancer.
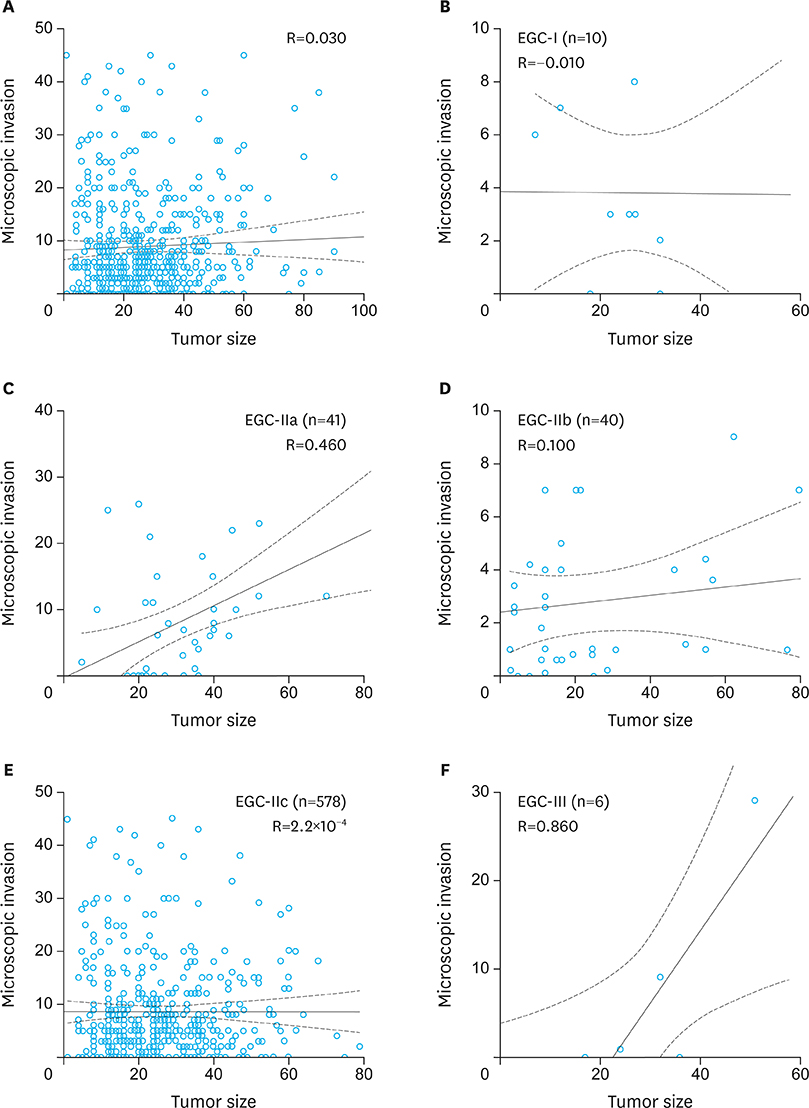
Fig. 3 Distribution of microscopic invasion according to tumor size in the risk group. (A) Entire risk group, (B) EGC-I, (C) EGC-IIa, (D) EGC-IIb, (E) EGC-IIc, and (F) EGC-III. Regression lines, CIs, and correlation coefficients (R) are displayed in the scatter plots. EGC = early gastric cancer; CI = confidence interval.
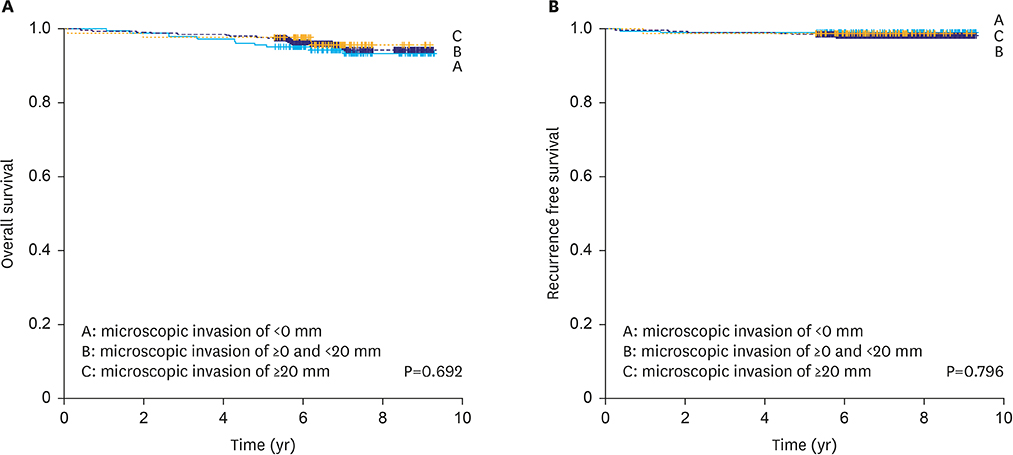
Fig. 4 Survival analysis according to microscopic invasion. (A) Overall survival (P=0.692). (B) Recurrence-free survival (P=0.796). Each line is presented safe group (microscopic invasion of <0 mm, n=186), microscopic invasion of ≥0 and <20 mm (n=588), and high-risk group (microscopic invasion of ≥20 mm, n=87).
Reference
-
1. Yang HK, Suh YS, Lee HJ. Minimally invasive approaches for gastric cancer-Korean experience. J Surg Oncol. 2013; 107:277–281.2. Suh YS, Yang HK. Screening and early detection of gastric cancer: East versus West. Surg Clin North Am. 2015; 95:1053–1066.3. Raziee HR, Cardoso R, Seevaratnam R, Mahar A, Helyer L, Law C, et al. Systematic review of the predictors of positive margins in gastric cancer surgery and the effect on survival. Gastric Cancer. 2012; 15:Suppl 1. S116–S124.4. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer. 2017; 20:1–19.5. National Comprehensive Cancer Network (US). NCCN Clinical Practice Guidelines in Oncology. Gastric Cancer, Version 2.2017. Fort Washington (PA): National Comprehensive Cancer Network;2017.6. Chen XZ, Zhang WH, Hu JK. Individualized proximal margin for early gastric cancer patients. World J Gastroenterol. 2014; 20:16793–16794.7. Kim BS, Oh ST, Yook JH, Kim HS, Lee IS, Kim BS. Appropriate gastrectomy resection margins for early gastric carcinoma. J Surg Oncol. 2014; 109:198–201.8. Squires MH 3rd, Kooby DA, Poultsides GA, Pawlik TM, Weber SM, Schmidt CR, et al. Is it time to abandon the 5-cm margin rule during resection of distal gastric adenocarcinoma? A multi-institution study of the U.S. Gastric Cancer Collaborative. Ann Surg Oncol. 2015; 22:1243–1251.9. Luo Y, Gao P, Song Y, Sun J, Huang X, Zhao J, et al. Clinicopathologic characteristics and prognosis of Borrmann type IV gastric cancer: a meta-analysis. World J Surg Oncol. 2016; 14:49.10. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, et al. AJCC Cancer Staging Manual. 7th ed. New York (NY): Springer;2010.11. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.12. Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System. 4th ed. Lyon: IARC Press;2010.13. Lee JH, Kim YI. Which is the optimal extent of resection in middle third gastric cancer between total gastrectomy and subtotal gastrectomy? J Gastric Cancer. 2010; 10:226–233.14. Ryu KW, Lee JH, Choi IJ, Bae JM. Preoperative endoscopic clipping: localizing technique of early gastric cancer. J Surg Oncol. 2003; 82:75–77.15. Park DJ, Lee HJ, Kim SG, Jung HC, Song IS, Lee KU, et al. Intraoperative gastroscopy for gastric surgery. Surg Endosc. 2005; 19:1358–1361.16. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003; 58:S3–S43.17. Ang TL, Fock KM, Teo EK, Tan J, Poh CH, Ong J, et al. The diagnostic utility of narrow band imaging magnifying endoscopy in clinical practice in a population with intermediate gastric cancer risk. Eur J Gastroenterol Hepatol. 2012; 24:362–367.18. Eleftheriadis N, Inoue H, Ikeda H, Onimaru M, Yoshida A, Maselli R, et al. Effective optical identification of type “0-IIb” early gastric cancer with narrow band imaging magnification endoscopy, successfully treated by endoscopic submucosal dissection. Ann Gastroenterol. 2015; 28:72–80.19. Aquino PF, Fischer JS, Neves-Ferreira AG, Perales J, Domont GB, Araujo GD, et al. Are gastric cancer resection margin proteomic profiles more similar to those from controls or tumors? J Proteome Res. 2012; 11:5836–5842.20. Woo JW, Ryu KW, Park JY, Eom BW, Kim MJ, Yoon HM, et al. Prognostic impact of microscopic tumor involved resection margin in advanced gastric cancer patients after gastric resection. World J Surg. 2014; 38:439–446.21. Lee JH, Ahn SH, Park DJ, Kim HH, Lee HJ, Yang HK. Clinical impact of tumor infiltration at the transected surgical margin during gastric cancer surgery. J Surg Oncol. 2012; 106:772–776.22. Squires MH 3rd, Kooby DA, Pawlik TM, Weber SM, Poultsides G, Schmidt C, et al. Utility of the proximal margin frozen section for resection of gastric adenocarcinoma: a 7-Institution Study of the US Gastric Cancer Collaborative. Ann Surg Oncol. 2014; 21:4202–4210.23. Information Committee of Korean Gastric Cancer Association. Korean Gastric Cancer Association nationwide survey on gastric cancer in 2014. J Gastric Cancer. 2016; 16:131–140.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Macroscopic Serosal Invasion in Advanced Gastric Cancer
- Risk Factors Affecting Lymph Node Metastasis and Recurrence in Early Gastric Cancer
- Factors Affecting Prognosis in Early Gastric Cancer
- Prognostic Factors on Overall Survival in Lymph Node Negative Gastric Cancer Patients Who Underwent Curative Resection
- Factors Affecting the Diagnostic Accuracy of Endoscopic Ultrasonography for the Depth of Invasion in Early Gastric Cancer
