Yonsei Med J.
2008 Feb;49(1):159-162.
Successful Etanercept Therapy for Refractory Sacroiliitis in a Patient with Ankylosing Spondylitis and Mixed Connective Tissue Disease
- Affiliations
-
- 1Department of Diagnostic Radiology, College of Medicine, Dankook University, Cheonan, Korea. kimsk714@cu.ac.kr
- 2Chang Hyn Kyu Rheumatism Clinic, Cheonan, Korea.
- 3Department of Internal Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea.
Abstract
- The concurrence of ankylosing spondylitis (AS) in a patient with mixed connective tissue disease (MCTD) is rarely described in the literature. Significant and sustained efficacy with tumor necrosis factor (TNF)-alpha blockers has been demonstrated in AS patients. However, evidence to date has revealed associated side effects, including antinuclear antibody induction and development of a lupus-like syndrome. Several authors have reported lupus-like manifestations in MCTD patients treated with TNF-alpha blockers used to control peripheral polyarthritis. In our case report, we demonstrate a good response to etanercept therapy for refractory sacroiliitis in a patient with coexisting AS and MCTD, without development of a lupus-like syndrome. This demonstrates that etanercept therapy may be an appropriate therapeutic agent for sacroiliitis in MCTD patients, as it is in AS alone.
MeSH Terms
-
Female
Humans
Immunoglobulin G/*therapeutic use
Magnetic Resonance Imaging
Middle Aged
Mixed Connective Tissue Disease/complications/*drug therapy/*pathology
Receptors, Tumor Necrosis Factor/*therapeutic use
Sacroiliac Joint/*drug effects/*pathology
Spondylitis, Ankylosing/complications/*drug therapy/*pathology
Treatment Outcome
Figure
-
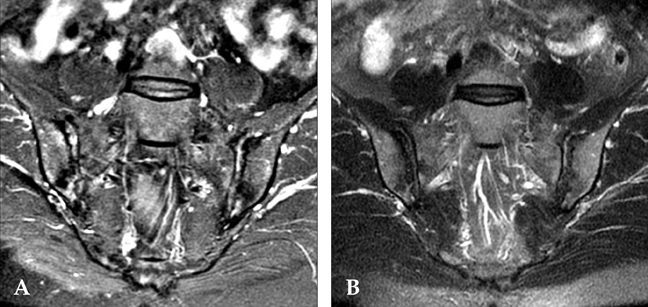
Fig. 1 (A) Magnetic resonance coronal fat suppressed T2-weighted image (WI) of both sacroiliac joints showing increased signal intensity within the joint spaces and subchondral marrow edema. Also present are subchondral erosions and localized fat deposition in the subchondral marrow spaces. (B) After 18 months, significant improvement of joint spaces with high signal intensity on fat-suppressed T2-WI with subchondral marrow edema identified at the same level.
Reference
-
1. Sharp GC, Irvin WS, Tan EM, Gould RG, Holman HR. Mixed connective tissue disease--an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972. 52:148–159.
Article2. Alarcón-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. Study of 593 patients. J Rheumatol. 1989. 16:328–334.3. Lee JK, Jung SS, Kim TH, Jun JB, Yoo DH, Kim SY. Coexistence of ankylosing spondylitis and mixed connective tissue disease in a single patient. Clin Exp Rheumatol. 1999. 17:263.4. Brandt J, Maier T, Rudwaleit M, Kühl U, Hiepe F, Sieper J, et al. Co-occurrence of spondyloarthropathy and connective tissue disease: development of Sjögren's syndrome and mixed connective tissue disease (MCTD) in a patient with ankylosing spondylitis. Clin Exp Rheumatol. 2002. 20:80–84.5. Richez C, Blanco P, Dumoulin C, Schaeverbeke T. Lupus erythematosus manifestations exacerbated by etanercept therapy in a patient with mixed connective tissue disease. Clin Exp Rheumatol. 2005. 23:273.6. Christopher-Stine L, Wigley F. Tumor necrosis factor-alpha antagonists induce lupus-like syndrome in patients with scleroderma overlap/mixed connective tissue disease. J Rheumatol. 2003. 30:2725–2727.7. Braun J, Brandt J, Listing J, Zink A, Alten R, Golder W, et al. Treatment of active ankylosing spondylitis with infliximab: a randomised controlled multicentre trial. Lancet. 2002. 359:1187–1193.
Article8. Brandt J, Khariouzov A, Listing J, Haibel H, Sörensen H, Grassnickel L, et al. Six-month results of a double-blind, placebo-controlled trial of etanercept treatment in patients with active ankylosing spondylitis. Arthritis Rheum. 2003. 48:1667–1675.
Article9. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984. 27:361–368.10. Alarcon-Segovia D, Villareal M. Kasukawa R, Sharp GC, editors. Classification and diagnostic criteria for mixed connective tissue disease. Mixed Connective Tissue Disease and Anti-nuclear Antibodies. 1987. Amsterdam: Elsevier;33–40.11. Brandt J, Rudwaleit M, Eggens U, Mertz A, Distler A, Sieper J, et al. Increased frequency of Sjögren's syndrome in patients with spondyloarthropathy. J Rheumatol. 1998. 25:718–724.12. Scotto di Fazano C, Grilo RM, Vergne P, Coyral D, Inaoui R, Bonnet C, et al. Is the relationship between spondyloarthropathy and Sjögren's syndrome in women coincidental? A study of 13 cases. Joint Bone Spine. 2002. 69:383–387.
Article13. Kim P, Grossman JM. Treatment of mixed connective tissue disease. Rheum Dis Clin North Am. 2005. 31:549–565. viii
Article14. Scott DL, Kingsley GH. Tumor necrosis factor inhibitors for rheumatoid arthritis. N Engl J Med. 2006. 355:704–712.
Article15. Shanahan JC, St Clair W. Tumor necrosis factor-alpha blockade: a novel therapy for rheumatic disease. Clin Immunol. 2002. 103:231–242.16. Rudwaleit M, Baraliakos X, Listing J, Brandt J, Sieper J, Braun J. Magnetic resonance imaging of the spine and the sacroiliac joints in ankylosing spondylitis and undifferentiated spondyloarthritis during treatment with etanercept. Ann Rheum Dis. 2005. 64:1305–1310.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ankylosing Spondylitis Accompanying Sarcoidosis
- CT Evaluation of Sacroiliitis' Differentiation of Infectious Sacroiliitis versus Ankylosing Spondylitis
- TNF Inhibitors and Uveitis in Ankylosing Spondylitis
- Etanercept Treatment in Ankylosing Spondylitis Hip Lesions
- Sacroiliitis in ankylosing spondylitis: a comparison of radiography and scintigraphy
