Yonsei Med J.
2009 Apr;50(2):239-244.
The Characteristics of Acute Aortic Dissection among Young Chinese Patients: A Comparison between Marfan Syndrome and Non-Marfan Syndrome Patients
- Affiliations
-
- 1Department of Emergency Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan. doc50024@ndmctsgh.edu.tw
- 2Department of Pediatric, Taoyuan Armed Force General Hospital, Taoyuan, Taiwan.
Abstract
- PURPOSE
Aortic dissection (AoD) is one of the most common catastrophes involving the aorta. Nevertheless, early diagnosis remains to be a challenge in the Emergency Department (ED), particularly in young individuals. In this study, we attempted to identify the characteristics of acute AoD among young individuals, particular in patients with Marfan syndrome. MATERIALS AND METHODS: This was an retrospective chart-review study conducted in a tertiary referring hospital. The hospital database was queried for the combination of AoD and patients under age of 40 years. The medical charts were reviewed to obtain demographic data, clinical data and laboratory characteristics by using a standardized data collection sheet. A comparison between Marfan syndrome and non-Marfan syndrome patients was performed. RESULTS: During the 10-years period, 18 of 344 patients with acute AoD were younger than 40 years-old. Patients with Marfan syndrome developed acute AoD at a younger age than patients without Marfan syndrome. The mean diastolic blood pressure was significantly lower in patients with Marfan syndrome upon presenting to the ED than those without. Patients with Marfan syndrome had trends toward higher risk of development of type A AoD, increased recurrence rate and higher mortality rate than those without. However, statistical significance was not present. CONCLUSION: ED physicians should have high alert to acute AoD in young patients presenting with severe unexplained chest and back pain, particularly in those patients with a history of heart diseases, hypertension, and Marfan syndrome or featuring Marfanoid habitus. Acute coronary syndrome, unexplained abdominal symptoms, and sudden cardiac arrest could be the initial manifestation of AoD in young patients. A low threshold to perform enhanced computed tomography may facilitate early diagnosis and timely treatment in this patient population.
MeSH Terms
-
Adult
Aneurysm, Dissecting/*complications/epidemiology/*pathology
Aortic Aneurysm/complications/epidemiology/*pathology
Asian Continental Ancestry Group
Female
Heart Defects, Congenital/complications/physiopathology
Humans
Hypertension/complications/physiopathology
Male
Marfan Syndrome/*complications/*physiopathology
Middle Aged
Retrospective Studies
Young Adult
Figure
-
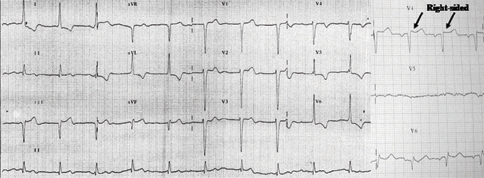
Fig. 1 Twelve-lead electrocardiography of patient No. 12 obtained in the emergency department. Note ST elevation in Lead II, III, aVF, reciprocal changes in I and aVL, and ST elevation in the rV4 (arrow) as well as high degree of AV block, findings consistent with acute inferio-posterior wall myocardial infarction.
Reference
-
1. Blanchard DG, Kimura BJ, Dittrich HC, DeMaria AN. Transesophageal echocardiography of the aorta. JAMA. 1994. 272:546–551.
Article2. Fuster V, Andrews P. Medical treatment of the aorta. I. Cardiol Clin. 1999. 17:697–715.
Article3. Fann JI, Smith JA, Miller DC, Mitchell RS, Moore KA, Grunkemeier G, et al. Surgical management of aortic dissection during a 30-year period. Circulation. 1995. 92(9):Suppl. II113–II121.
Article4. Meszaros I, Mórocz J, Szlávi J, Schmidt J, Tornóci L, Nagy L, et al. Epidemiology and clinicopathology of aortic dissection. Chest. 2000. 117:1271–1278.
Article5. Fikar CR, Koch S. Etiologic factors of acute aortic dissection in children and young adults. Clin Pediatr (Phila). 2000. 39:71–80.
Article6. Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Shumway NE. Management of acute aortic dissections. Ann Thorac Surg. 1970. 10:237–247.
Article7. De Paepe A, Devereux RB, Dietz HC, Hennekam RC, Pyeritz RE. Revised diagnostic criteria for the Marfan syndrome. Am J Med Genet. 1996. 62:417–426.
Article8. Summers KM, West JA, Peterson MM, Stark D, McGill JJ, West MJ. Challenges in the diagnosis of Marfan syndrome. Med J Aust. 2006. 184:627–631.
Article9. Januzzi JL, Isselbacher EM, Fattori R, Cooper JV, Smith DE, Fang J, et al. Characterizing the young patients with aortic dissection: results from the International Registry of Aortic Dissection (IRAD). J Am Coll Cardiol. 2004. 43:665–669.
Article10. Januzzi JL, Marayati F, Mehta RH, Cooper JV, O'Gara PT, Sechtem U, et al. Comparison of aortic dissection in patients with and without Marfan's syndrome (results from the International Registry of Aortic Dissection). Am J Cardiol. 2004. 94:400–402.
Article11. Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002. 122:311–328.
Article12. Suzuki T, Mehta RH, Ince H, Nagai R, Sakomura Y, Weber F, et al. Clinical profiles and outcomes of acute type B aortic dissection in the current era: lessons from the International Registry of Aortic Dissection (IRAD). Circulation. 2003. 108:suppl 1. II312–II317.
Article13. Crawford ES. The diagnosis and management of aortic dissection. JAMA. 1990. 264:2537–2541.
Article14. Spittell PC, Spittell JA Jr, Joyce JW, Tajik AJ, Edwards WD, Schaff HV, et al. Clinical features and differential diagnosis of aortic dissection: experience with 236 cases (1980 through 1990). Mayo Clin Proc. 1993. 68:642–651.
Article15. Smith JA, Fann JI, Miller DC, Moore KA, DeAnda A Jr, Mitchell RS, et al. Surgical management of aortic dissection in patients with the Marfan syndrome. Circulation. 1994. 90:II235–II242.16. Ramires F, Godfrey M, Lee B, Tsipouras P. Scriver CR, Beaudet AI, Sly WS, Valle D, editors. Marfan syndrome and related disorders. The metabolic and molecular bases of inherited disease. 1995. Volume 3:7th ed. New York: McGraw Hill;4079–4094.17. Tsementzis SA, Gill JS, Hitchcock ER, Gill SK, Beevers DG. Diurnal variation of and activity during the onset of stroke. Neurosurgery. 1985. 17:901–904.
Article18. Kojima S, Sumiyoshi M, Nakata Y, Daida H. Triggers and circadian distribution of the onset of acute aortic dissection. Circ J. 2002. 66:232–235.
Article19. Gwan-Nulla DN, Davidson WR Jr, Grenko RT, Damiano RJ Jr. Aortic dissection in a weight lifter with nodular fasciitis of the aorta. Ann Thorac Surg. 2000. 69:1931–1932.
Article20. de Virgilio C, Nelson RJ, Milliken J, Snyder R, Chiang F, MacDonald WD, et al. Ascending aortic dissection in weight lifters with cystic medial degeneration. Ann Thorac Surg. 1990. 49:638–642.
Article21. Baumgartner FJ, Omari BO, Robertson JM. Weight lifting, Marfan's syndrome, and acute aortic dissection. Ann Thorac Surg. 1997. 64:1871–1872.22. Rashid J, Eisenberg MJ, Topol EJ. Cocaine-induced aortic dissection. Am Heart J. 1996. 132:1301–1304.
Article23. Li W, Su J, Sehgal S, Altura BT, Altura BM. Cocaine-induced relaxation of isolated rat aortic rings and mechanisms of action: possible relation to cocaine-induced aortic dissection and hypotension. Eur J Pharmacol. 2004. 496:151–158.
Article24. Papadimos TJ, Hofmann JP. Aortic dissection after forceful coughing. Anaesthesia. 2006. 61:71–72.
Article25. Buda AJ, Pinsky MR, Ingels NB Jr, Daughters GT 2nd, Stinson EB, Alderman EL. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med. 1979. 301:453–459.
Article26. Virolainen J, Kupari M. Age-dependent increase in aortic stiffness during negative intrathoracic pressure in healthy subjects. Am J Cardiol. 1993. 71:878–882.
Article27. Jagannath AS, Sos TA, Lockhart SH, Saddekni S, Sniderman KW. Aortic dissection: a statistical analysis of the usefulness of plain chest radiographic findings. AJR Am J Roentgenol. 1986. 147:1123–1126.
Article28. Moore AG, Eagle KA, Bruckman D, Moon BS, Malouf JF, Fattori R, et al. Choice of computed tomography, transesophageal echocardiography, magnetic resonance imaging, and aortography in acute aortic dissection: International Registry of Acute Aortic Dissection (IRAD). Am J Cardiol. 2002. 89:1235–1238.
Article29. Hayter RG, Rhea JT, Small A, Tafazoli FS, Novelline RA. Suspected aortic dissection and other aortic disorders: multi-detector row CT in 373 cases in the emergency setting. Radiology. 2006. 238:841–852.
Article30. Yoshida S, Akiba H, Tamakawa M, Yama N, Hareyama M, Morishita K, et al. Thoracic involvement of type A aortic dissection and intramural hematoma: diagnostic accuracy--comparison of emergency helical CT and surgical findings. Radiology. 2003. 228:430–435.
Article31. Akutsu K, Sato N, Yamamoto T, Morita N, Takagi H, Fujita N, et al. A rapid bedside D-dimer assay (cardiac D-dimer) for screening of clinically suspected acute aortic dissection. Circ J. 2005. 69:397–403.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Aortic Dissection in Pregnancy with the Marfan Syndrome
- A Case Report of Acute Type II Aortic Dissection in a Patient with Marfan's Syndrome and Who Was 24 Weeks Pregnant: A case report
- A Case of Marfan Syndrome in Pregnancy with Aortic Root Dilatation
- Acute Type II Aortic Dissection with Severe Aortic Regurgitation and Chronic Descending Aortic Dissection in Pregnant Patient with Marfan Syndrome
- A Case of Dissection in Marfan Syndrome with Ascending Aortic Aneurysm
