Long-Term Results after Surgical Treatment of Ebstein's Anomaly: a 30-year Experience
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul, Korea. kyj@plaza.snu.ac.kr
- KMID: 2389629
- DOI: http://doi.org/10.4070/kcj.2016.46.5.706
Abstract
- BACKGROUND AND OBJECTIVES
The aim of the study is to evaluate the long-term results after a surgical repair of Ebstein's anomaly.
SUBJECTS AND METHODS
Forty-eight patients with Ebstein's anomaly who underwent open heart surgery between 1982 and 2013 were included. Median age at operation was 5.6 years (1 day-42.1 years). Forty-five patients (93.7%) demonstrated tricuspid valve (TV) regurgitation of less than moderate degree. When the patients were divided according to Carpentier's classification, types A, B, C, and D were 11, 21, 12, and 4 patients, respectively. Regarding the type of surgical treatment, bi-ventricular repair (n=38), one-and-a half ventricular repair (n=5), and single ventricle palliation (n=5) were performed. Of 38 patients who underwent a bi-ventricular repair, TV repairs were performed by Danielson's technique (n=20), Carpentier's technique (n=11), Cone repair (n=4), and TV annuloplasty (n=1). Two patients underwent TV replacement. Surgical treatment strategies were different according to Carpentier's types (p<0.001) and patient's age (p=0.022).
RESULTS
There were 2 in-hospital mortalities (4.2%; 1 neonate and 1 infant) and 2 late mortalities during follow-up. Freedom from recurrent TV regurgitation rates at 5, 10, and 15 years were 88.6%, 66.3%, 52.7%, respectively. TV regurgitation recurrence did not differ according to surgical method (p=0.800). Survival rates at 5, 10, and 20 years were 95.8%, 95.8%, and 85.6%, respectively, and freedom from reoperation rates at 5, 10, and 15 years were 85.9%, 68.0%, and 55.8%, respectively.
CONCLUSION
Surgical treatment strategies were decided according to Carpentier's type and patient's age. Overall survival and freedom from reoperation rates at 10 years were 95.8% and 68.0%, respectively. Approximately 25% of patients required a second operation for TV during the follow-up.
Keyword
MeSH Terms
Figure
-
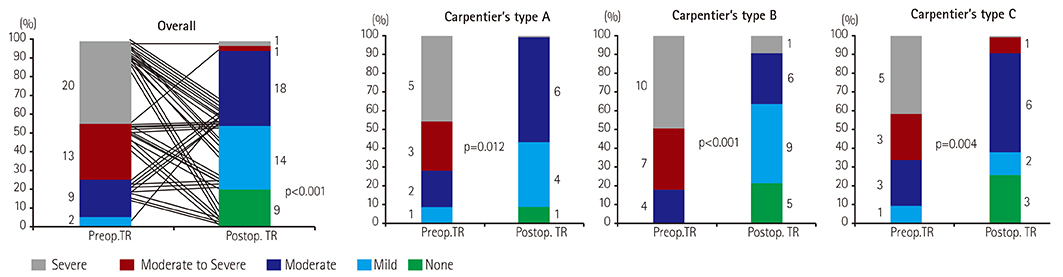
Fig. 1 Comparison of severity of TR. Number of patients according to the severity of TR before and after the repair is shown in graph. The severity of TR was also compared according to the Carpentier's type. TR: tricuspid regurgitation.
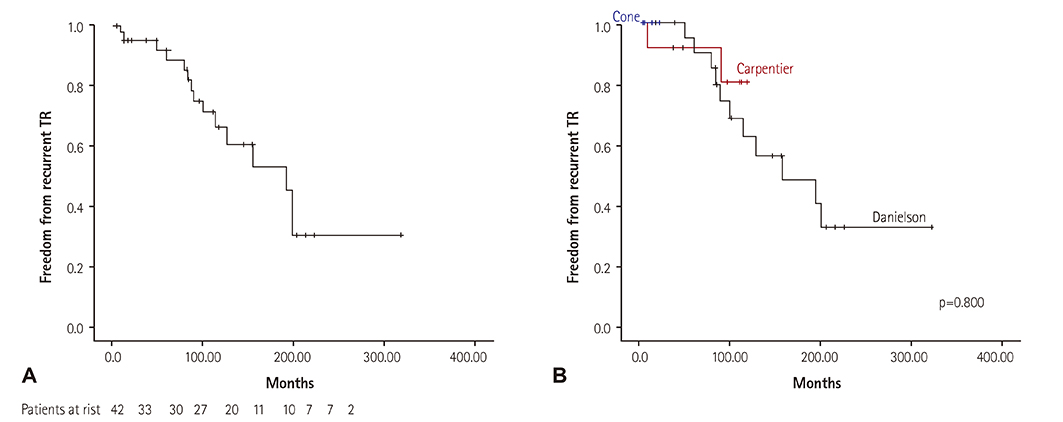
Fig. 2 Kaplan-Meier estimated overall freedom from recurrent TR (A). Freedom from recurrent TR rates at 5, 10, and 15 years were 88.6%, 66.3%, and 52.7%, respectively. Kaplan-Meier estimated freedom from recurrent TR according to surgical strategies (B). Log-rank test showed no significant difference in recurrent TR rates between surgical strategies (Danielson repair, Carpentier repair, and cone repair). TR: tricuspid regurgitation.
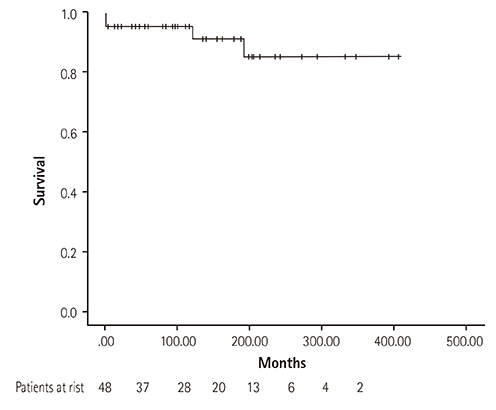
Fig. 3 Kaplan-Meier estimated survival after surgical repair of Ebstein's anomaly.
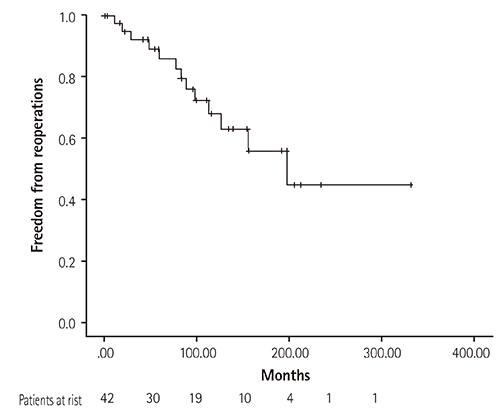
Fig. 4 Kaplan-Meier estimated freedom from reoperations after initial surgical repair of Ebstein's anomaly.
Reference
-
1. Attenhofer Jost CH, Connolly HM, Edwards WD, Hayes D, Warnes CA, Danielson GK. Ebstein's anomaly - review of a multifaceted congenital cardiac condition. Swiss Med Wkly. 2005; 135:269–281.2. Krieger EV, Valente AM. Diagnosis and management of ebstein anomaly of the tricuspid valve. Curr Treat Options Cardiovasc Med. 2012; 14:594–607.3. Attenhofer Jost CH, Connolly HM, Dearani JA, Edwards WD, Danielson GK. Ebstein's anomaly. Circulation. 2007; 115:277–285.4. Huang CJ, Chiu IS, Lin FY, et al. Role of electrophysiological studies and arrhythmia intervention in repairing Ebstein's anomaly. Thorac Cardiovasc Surg. 2000; 48:347–350.5. Iturralde P, Nava S, Sálica G, Medeiros A, et al. Electrocardiographic characteristics of patients with Ebstein's anomaly before and after ablation of an accessory atrioventricular pathway. J Cardiovasc Electrophysiol. 2006; 17:1332–1336.6. Khositseth A, Danielson GK, Dearani JA, Munger TM, Porter CJ. Supraventricular tachyarrhythmias in Ebstein anomaly: management and outcome. J Thorac Cardiovasc Surg. 2004; 128:826–833.7. Paranon S, Acar P. Ebstein's anomaly of the tricuspid valve: From fetus to adult. Heart. 2008; 94:237–243.8. Carpentier A, Chauvaud S, Macé L, et al. A new reconstructive operation for ebstein's anomaly of the tricuspid valve. J Thorac Cardiovasc Surg. 1988; 96:92–101.9. Stulak JM, Dearani JA, Danielson GK. Surgical management of ebstein's anomaly. Semin Thorac Cardiovasc Surg Pediatr Card Surg Ann. 2007; 10:105–111.10. Davies RR, Pasquali SK, Jacobs ML, Jacobs JJ, Wallace AS, Pizarro C. Current spectrum of surgical procedures performed for Ebstein's malformation : An analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. Ann Thorac Surg. 2013; 96:1703–1710.11. Hunter SW, Lillehei CW. Ebstein's malformation of the tricuspid valve: Study of a case together with suggestion of a new form of surgical therapy. Dis Chest. 1958; 33:297–304.12. Hardy K, May IA, Webster CA, Kimball KG. Ebstein's anomaly: A functional concept and successful definitive repair. J Thorac Cardiovasc Surg. 1964; 48:927–940.13. Danielson GK, Driscoll DJ, Mair DD, Warnes CA, Oliver WC Jr. Operative treatment of ebstein's anomaly. J Thorac Cardiovasc Surg. 1992; 104:1195–1202.14. Silva JP, Baumgratz JF, Fonseca Ld, et al. Ebstein's anomaly: Results of the conic reconstruction of the tricuspid valve. Arq Bras Cardiol. 2004; 82:212–216.15. Oxenius A, Attenhofer Jost CH, Prêtre R, et al. Management and outcome of Ebstein's anomaly in children. Cardiol Young. 2013; 23:27–34.16. Raju V, Dearani JA, Burkhart HM, et al. Right ventricular unloading for heart failure related to Ebstein malformation. Ann Thorac Surg. 2014; 98:167–174. discussion 173-4.17. Jaquiss RD, Imamura M. Management of Ebstein's anomaly and pure tricuspid insufficiency in the neonate. Semin Thorac Cardiovasc Surg. 2007; 19:258–263.18. Muraru D, Surkova E, Badano LP. Current trends in the diagnosis and management of functional tricuspid regurgitation. Korean Circ J. 2016; 46:e101.19. Cheung YF. Functional assessment for congenital heart disease. Korean Circ J. 2014; 44:59–73.20. Celermajer DS, Bull C, Till JA, et al. Ebstein's anomaly: Presentation and outcome from fetus to adult. J Am Coll Cardiol. 1994; 23:170–176.21. Kapusta L, Eveleigh RM, Poulino SE, et al. Ebstein's anomaly: factors associated with death in childhood and adolescence: a multi-centre, long-term study. Eur Heart J. 2007; 28:2661–2666.22. Boston US, Dearani JA, O'Leary PW, Driscoll DJ, Danielson GK. Tricuspid valve repair for Ebstein's anomaly in young children: a 30-year experience. Ann Thorac Surg. 2006; 81:690–696. discussion 695-6.23. Chauvaud SM, Brancaccio G, Carpentier AF. Cardiac arrhythmia in patients undergoing surgical repair of ebstein's anomaly. Ann Thorac Surg. 2001; 71:1547–1552.24. Khositseth A, Danielson GK, Dearani JA, Munger TM, Porter CJ. Supraventricular tachyarrhythmias in Ebstein anomaly: management and outcome. J Thorac Cardiovasc Surg. 2004; 128:826–833.25. Brown ML, Dearani JA, Danielson GK, et al. The outcomes of operations for 539 patients with ebstein anomaly. J Thorac Cardiovasc Surg. 2008; 135:1120–1136.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cone Reconstruction for Tricuspid Valve Repair in a Patient with Ebstein's Anomaly : A case report
- A Modified Technique in Surgical Correction of Ebstein Anomaly
- Cone Repair in Adult Patients with Ebstein Anomaly
- Surgical treatment of isolated primary tricuspid insufficiency except Ebstein's anomaly: report of 2 cases
- Surgical Strategies in Ebstein's Anomaly: Surgical Treatments and Results
