Laparoscopic Distal Gastrectomy in a Patient with Situs Inversus Totalis: A Case Report
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea. hkyang@snu.ac.kr
- 2Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Radiology, Seoul National University Hospital, Seoul, Korea.
Abstract
- We report our experience with two cases of situs inversus totalis, both involving patients diagnosed with gastric cancer. These were a 52-year-old male with a preoperative staging of cT1bN0M0 and a 68-year-old male with a staging of cT2N0M0, both of whom underwent surgery. The former was found to have vascular anomalies in the preoperative computed tomography, so we performed a computed tomography angiography with three-dimensional reconstruction. Laparoscopy-assisted distal gastrectomy with Billroth I anastomosis was performed with D1+ lymph node dissection, and a small laparotomy was made for extracorporeal anastomosis. In contrast, the latter case showed no vascular anomalies in the preoperative computed tomography, and totally laparoscopic distal gastrectomy with delta anastomosis was performed with D1+ lymph node dissection. There were no intraoperative problems in either patient and they were discharged without postoperative complications. Histopathological examination revealed a poorly differentiated adenocarcinoma (pT2N0M0) and a well-differentiated adenocarcinoma (pT1aN0M0), respectively.
Keyword
MeSH Terms
Figure
-
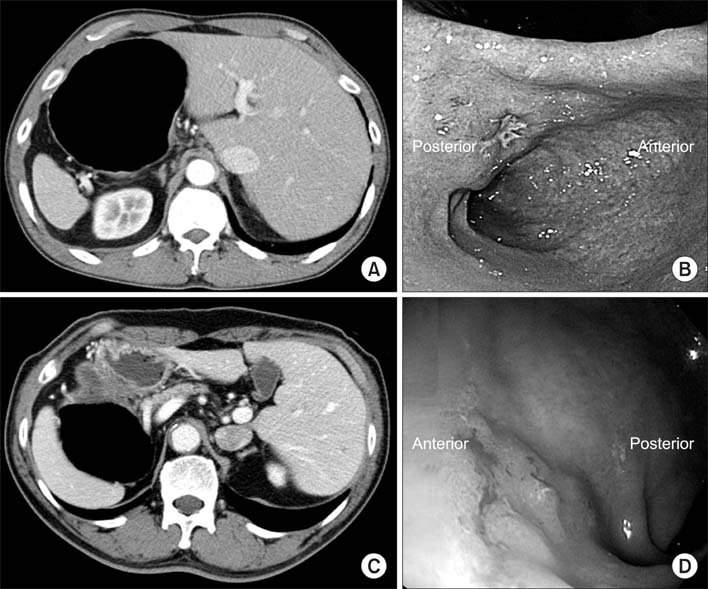
Fig. 1 Computed tomography showing transposition of the abdominal organs in case 1 (A), and case 2 (C). (B, D) Esophagogastroduodenoscopy image showing the lesion on the mid antrum, lesser curvature in case 1 (B), and on the mid antrum, anterior wall in case 2 (D).
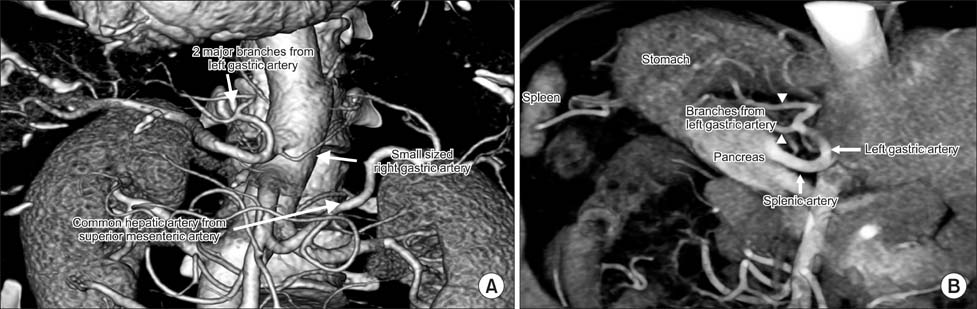
Fig. 2 Case 1. Three-dimensional reconstruction image of computed tomography angiography showing two branches of the left gastric artery (arrowheads), right gastric artery from the celiac trunk, and replaced common hepatic artery from the superior mesenteric artery (A, B).
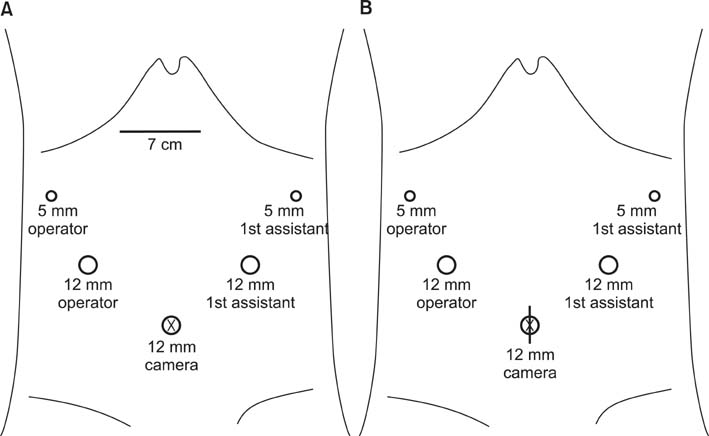
Fig. 3 The placement of ports in (A) case 1, (B) case 2. A 7 cm incision is made below the xyphoid process for extracorporeal anastomosis (A). An extension of the umbilical incision is made for specimen extraction only (B).
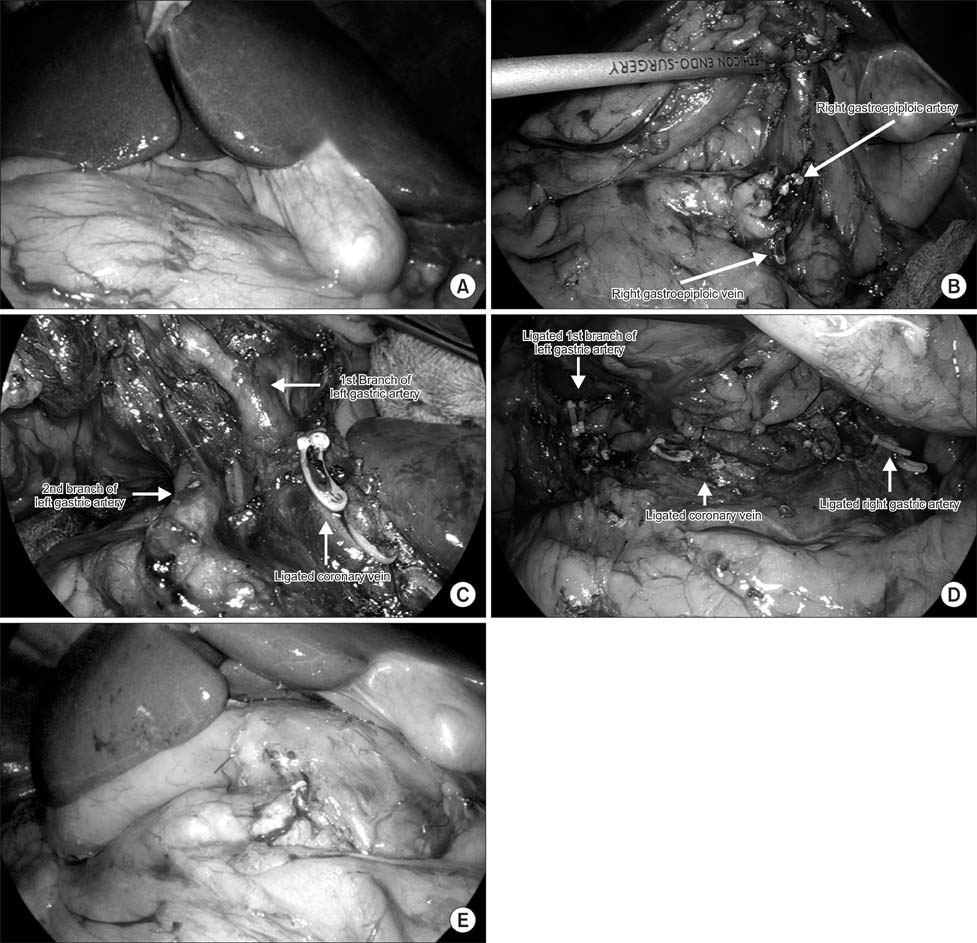
Fig. 4 Case 1. (A) Initial laparoscopic view showing transposition of abdominal organs. (B) The ligated right gastroepiploic artery and vein. The ligated coronary vein. (C) Anatomic variation in the 1st and 2nd branch of the left gastric artery is apparent. (D) The ligated 1st branch of the left gastric artery, right gastric artery and coronary vein. (E) The wound after Billroth I anastomosis and Fibrin glue had been applied.

Fig. 5 Case 2. (A) Initial laparoscopic view showing transposition of abdominal organs. (B) Ligated right gastroepiploic artery and vein. (C) Suprapancreatic lymph node dissection with ligated left gastric artery. (D) After delta-shaped anastomosis.
Reference
-
1. Iwamura T, Shibata N, Haraguchi Y, Hisashi Y, Nishikawa T, Yamada H, et al. Synchronous double cancer of the stomach and rectum with situs inversus totalis and polysplenia syndrome. J Clin Gastroenterol. 2001; 33:148–153.
Article2. Yamaguchi S, Orita H, Yamaoka T, Mii S, Sakata H, Hashizume M. Laparoscope-assisted distal gastrectomy for early gastric cancer in a 76-year-old man with situs inversus totalis. Surg Endosc. 2003; 17:352–353.
Article3. Yang HK, Lee HJ, Ahn HS, Yoo MW, Lee IK, Lee KU. Safety of modified double-stapling end-to-end gastroduodenostomy in distal subtotal gastrectomy. J Surg Oncol. 2007; 96:624–629.
Article4. Shabbir A, Lee JH, Lee MS, Park do J, Kim HH. Combined suture retraction of the falciform ligament and the left lobe of the liver during laparoscopic total gastrectomy. Surg Endosc. 2010; 24:3237–3240.
Article5. Kanaya S, Kawamura Y, Kawada H, Iwasaki H, Gomi T, Satoh S, et al. The delta-shaped anastomosis in laparoscopic distal gastrectomy: analysis of the initial 100 consecutive procedures of intracorporeal gastroduodenostomy. Gastric Cancer. 2011; 14:365–371.
Article6. Yoshida Y, Saku M, Masuda Y, Maekawa S, Ikejiri K, Furuyama M. Total gastrectomy for gastric cancer associated with situs inversus totalis. A report of 2 cases. S Afr J Surg. 1992; 30:156–158.7. Allen FRWK. A case of malignant tumor of the stomach in a male with transposition of the viscera. Ind Med Gaz. 1936; 71:32.8. Futawatari N, Kikuchi S, Moriya H, Katada N, Sakuramoto S, Watanabe M. Laparoscopy-assisted distal gastrectomy for early gastric cancer with complete situs inversus: report of a case. Surg Today. 2010; 40:64–67.
Article9. Sano T, Aiko T. New Japanese classifications and treatment guidelines for gastric cancer: revision concepts and major revised points. Gastric Cancer. 2011; 14:97–100.
Article10. Kang BH, Lee SL, Hur H, Kim JY, Cho YK, Han SU. Laparoscopy assisted subtotal gastrectomy in gastric cancer patient with situs inversus in Korea. J Korean Surg Soc. 2010; 79:513–517.
Article11. Kim HB, Lee JH, Park do J, Lee HJ, Kim HH, Yang HK. Robot-assisted distal gastrectomy for gastric cancer in a situs inversus totalis patient. J Korean Surg Soc. 2012; 82:321–324.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Port Laparoscopic Cholecystectomy in a Patient with Situs Inversus Totalis: A Case Report
- Laparoscopic cholecystectomy in a case of situs inversus totalis: a review of technical challenges and adaptations
- Laparoscopic Low Anterior Resection in a Rectal Cancer Patient with Situs Inversus Totalis: A Case Report
- Radical Subtotal Gastrectomy in Early Gastric Cancer Patient with Situs Inversus Totalis
- Laparoscopy Assisted Subtotal Gastrectomy in Gastric Cancer Patient with Situs Inversus in Korea
