Nodo-Colonic Fistula Caused by Intra-Abdominal Tuberculous Lymphadenitis during Treatment with Anti-Tuberculous Medication: A Case Report
- Affiliations
-
- 1Department of Radiology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. s2671@paik.ac.kr
- KMID: 2344805
- DOI: http://doi.org/10.3348/jksr.2016.75.2.143
Abstract
- Recently, the overall incidence of tuberculosis has decreased, but the incidence of an extrapulmonary manifestation in patients with tuberculosis has increased in the Republic of Korea. Although intestinal tuberculosis is not infrequent, a fistula caused by tuberculosis is a rare condition. A 23-year-old man presented with fever, diarrhea and right lower quadrant pain. A computed tomography (CT) scan revealed a lobulated, peripherally enhancing, low density mass in the mesentery. The patient underwent laparoscopic biopsy for necrotic lymph node, and intra-abdominal tuberculous lymphadenitis was diagnosed. Four months after initiating treatment with anti-tuberculous medication, the patient developed fever together with lower abdominal pain. A follow-up CT scan revealed a fistulous tract that had developed between the initially noted lymphadenopathy and the proximal ascending colon. Laparoscopic right hemicolectomy was performed as a curative treatment. This case suggests that a nodo-colonic fistula may occur as a paradoxical response in patients with intra-abdominal tuberculous lymphadenitis during treatment with anti-tuberculous medication.
MeSH Terms
Figure
-
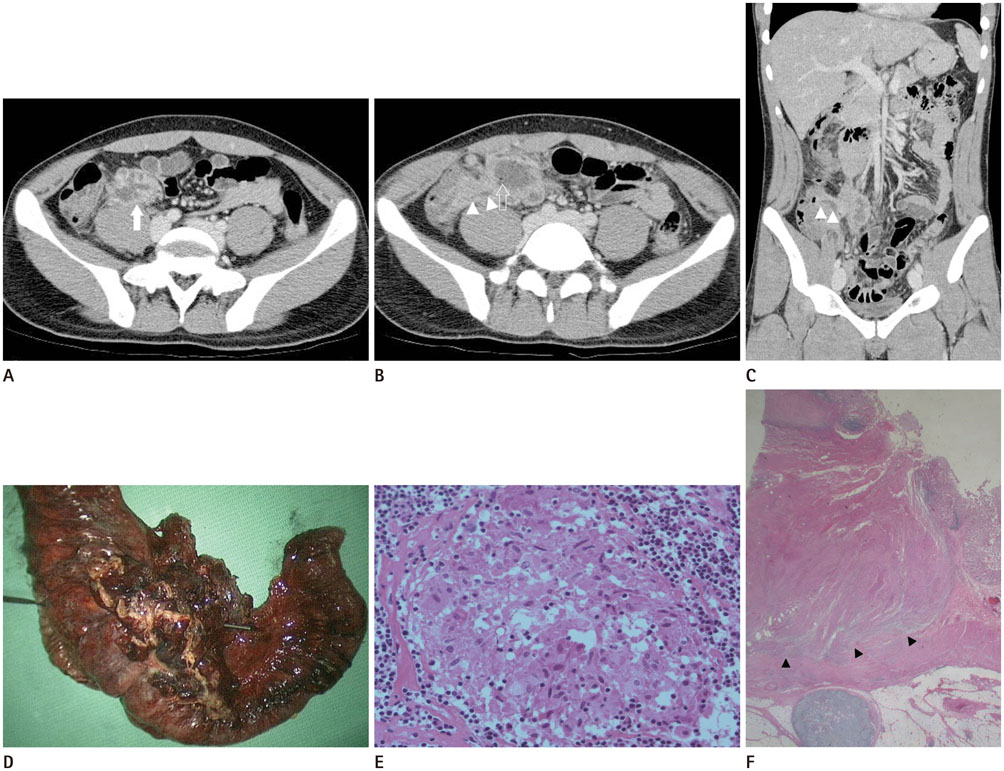
Fig. 1 A 23-year-old male patient with a diagnosis of intra-abdominal tuberculous lymphadenitis. A. Initial abdominal CT scan demonstrates a lobulated, peripherally enhancing low-density mass (arrow) in the mesentery of the right lower quadrant. B. Follow-up abdominal CT scan obtained four months later, shows an increase in the size of the mass, development of internal tiny air bubbles (empty arrow), and a fistulous tract (arrowheads). C. Coronal reconstructed CT scan shows a fistulous tract extending to the proximal ascending colon (arrowheads). D. Gross specimen obtained in the operation room shows a penetrating rod in accordance with the fistulous tract. E. Histopathologic feature on this photomicrograph shows a pink, amorphous region in the center of a granuloma ringed by epithelioid cells, suggesting caseous necrosis (hematoxylin-eosin stain; high power field). F. Another macroscopic view shows mural defects (arrowheads) suggesting fistula formation in the proximal ascending colon (hematoxylin-eosin stain; low power field). CT = computed tomography
Reference
-
1. Kwon DY, Park HW, Seo SH, Jang BK, Hwang JY, Lee JM, et al. A case of duodenal fistula caused by intestinal tuberculosis. Korean J Gastrointest Endosc. 2004; 28:131–135.2. Kim HJ. Current status of tuberculosis in Korea. Korean J Med. 2012; 82:257–262.3. Korea Centers for Disease Control and Prevention. Annual report on the notified tuberculosis in Korea, 2014. Notified tuberculosis status in Korea, 2014. Cheongju: Korea Centers for Disease Control and Prevention;2015.4. Burrill J, Williams CJ, Bain G, Conder G, Hine AL, Misra RR. Tuberculosis: a radiologic review. Radiographics. 2007; 27:1255–1273.5. Kim KS, Cha SH, Ahn JH, Cho MY. A large tuberculous abscess mimicking a retroperitoneal cystic mass: a case report. J Korean Soc Radiol. 2015; 72:202–205.6. Nagi B, Lal A, Kochhar R, Bhasin DK, Thapa BR, Singh K. Perforations and fistulae in gastrointestinal tuberculosis. Acta Radiol. 2002; 43:501–506.7. Lee KR, Seo KS, Cheo JH, Choi SC, Kim K, Yim YG, et al. A case of duodenal fistula caused by intra-abdominal tuberculous lymphadenopathy during anti-tuberculous medication. Korean J Gastrointest Endosc. 2008; 37:433–437.8. Lee DG, Kim GH. Nododuodenal fistula caused by tuberculosis. Korean J Intern Med. 2011; 26:477.9. Cho OH, Park KH, Kim T, Song EH, Jang EY, Lee EJ, et al. Paradoxical responses in non-HIV-infected patients with peripheral lymph node tuberculosis. J Infect. 2009; 59:56–61.10. Wong WM, Lai KC, Yiu WC, Wong BC, Chan FL, Lai CL. Intestinal tuberculosis mimicking fistulizing Crohn's disease. J Gastroenterol Hepatol. 2007; 22:137–139.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Duodenal Fistula Caused by Intra-abdominal Tuberculous Lymphadenopathy during Anti-tuberculous Medication
- Esophago-Mediastinal Fistula Due to Tuberculous Mediastinal Lymphadenitis
- Choledocho-duodenal Fistula Caused by Tuberculosis
- Polymicrobial Purulent Pericarditis Probably caused by a Broncho-Lymph Node-Pericardial Fistula in a Patient with Tuberculous Lymphadenitis
- A Case of Tuberculous Peritonitis Developed during Chemotherapy for Tuberculous Pleurisy as Paradoxical Response
