Remnant Pacemaker Lead Tips after Lead Extractions in Pacemaker Infections
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- KMID: 2344434
- DOI: http://doi.org/10.4070/kcj.2016.46.4.569
Abstract
- Complete hardware removal is recommended in the case of patients with cardiovascular implantable electronic device (CIED) infections. However, the complete extraction of chronically implanted leads is not always achieved. The outcomes and optimal management of CIED infections with retained material after lead extractions have not been elucidated. In this case report, we present five patients with CIED infections with remnant lead tips even after lead extractions. Two patients had localized pocket infections, and were managed with antibiotics for a period of more than two weeks. The other three patients had infective endocarditis, and were managed with antibiotics for a period of more than four weeks. In one patient, the lead tip migrated to the right pulmonary artery, but did not produce any symptoms or complications. Only one of five patients experienced a resurgence of an infection.
MeSH Terms
Figure
-
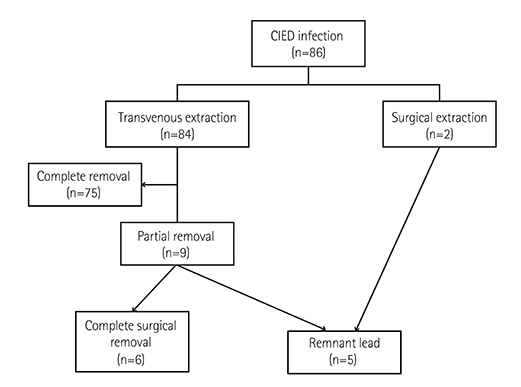
Fig. 1 Diagram representing the patients. CIED: cardiovascular implantable electronic device.
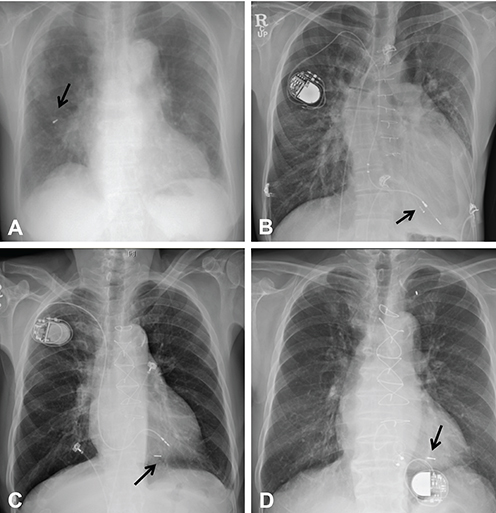
Fig. 2 Chest radiographs of four patients. (A) Embolization of the remnant lead tip (arrow) after lead extraction in Patient 1. (B) The remaining lead tip (arrow) after lead extraction in Patient 2. (C) The remnant lead tip (arrow) after lead extraction in Patient 3. A new pacemaker was implanted on the contralateral side. (D) The remnant lead tip (arrow) after lead extraction in Patient 4. A new epicardial pacemaker was implanted.
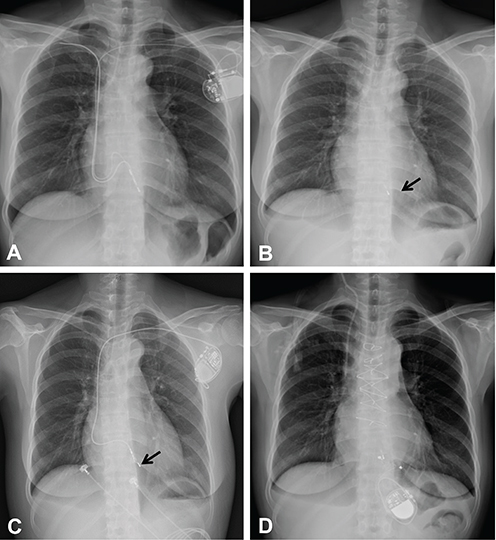
Fig. 3 Chest radiographs of patient 5. (A) The lead of the right sided pacemaker (generator removed previously): and the left sided VVI pacemaker. (B) The remnant lead tip (arrow) after lead extraction. (C) The remnant lead tip (arrow) and the VVI pacemaker implanted three months after lead extraction. (D) The newly implanted epicardial pacemaker after surgical removal. VVI: ventricular demand pacing.
Reference
-
1. Masoudi FA, Ponirakis A, Yeh RW, et al. Cardiovascular care facts: a report from the national cardiovascular data registry: 2011. J Am Coll Cardiol. 2013; 62:1931–1947.2. Greenspon AJ, Patel JD, Lau E, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J Am Coll Cardiol. 2011; 58:1001–1006.3. Victor F, De Place C, Camus C, et al. Pacemaker lead infection: echocardiographic features, management, and outcome. Heart. 1999; 81:82–87.4. Athan E, Chu VH, Tattevin P, et al. Clinical characteristics and outcome of infective endocarditis involving implantable cardiac devices. JAMA. 2012; 307:1727–1735.5. Baddour LM, Epstein AE, Erickson CC, et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation. 2010; 121:458–477.6. Wilkoff BL, Love CJ, Byrd CL, et al. Transvenous lead extraction: Heart Rhythm Society expert consensus on facilities, training, indications, and patient management: this document was endorsed by the American Heart Association (AHA). Heart Rhythm. 2009; 6:1085–1104.7. Byrd CL, Wilkoff BL, Love CJ, Sellers TD, Reiser C. Clinical study of the laser sheath for lead extraction: the total experience in the United States. Pacing Clin Electrophysiol. 2002; 25:804–808.8. Love CJ, Wilkoff BL, Byrd CL, et al. Recommendations for extraction of chronically implanted transvenous pacing and defibrillator leads: indications, facilities, training. North American Society of Pacing and Electrophysiology Lead Extraction Conference Faculty. Pacing Clin Electrophysiol. 2000; 23(4 Pt 1):544–551.9. Darouiche RO. Treatment of infections associated with surgical implants. N Engl J Med. 2004; 350:1422–1429.10. Klug D, Wallet F, Kacet S, Courcol RJ. Detailed bacteriologic tests to identify the origin of transvenous pacing system infections indicate a high prevalence of multiple organisms. Am Heart J. 2005; 149:322–328.11. Klug D, Wallet F, Lacroix D, et al. Local symptoms at the site of pacemaker implantation indicate latent systemic infection. Heart. 2004; 90:882–886.12. Robinson T, Oliver J, Sheridan P, Sahu J, Bowes R. Fragmentation and embolization of pacemaker leads as a complication of lead extraction. Europace. 2010; 12:754–755.13. Baddour LM, Bettmann MA, Bolger AF, et al. Nonvalvular cardiovascular device-related infections. Circulation. 2003; 108:2015–2031.14. Chua JD, Wilkoff BL, Lee I, Juratli N, Longworth DL, Gordon SM. Diagnosis and management of infections involving implantable electrophysiologic cardiac devices. Ann Intern Med. 2000; 133:604–608.15. Sohail MR, Uslan DZ, Khan AH, et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J Am Coll Cardiol. 2007; 49:1851–1859.16. Turkisher V, Priel I, Dan M. Successful management of an infected implantable cardioverter defibrillator with oral antibiotics and without removal of the device. Pacing Clin Electrophysiol. 1997; 20(9 Pt 1):2268–2270.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Infected Endocarditis Related Pacemaker leads: A Case Report
- Permanent Pacemaker Lead Induced Severe Tricuspid Regurgitation in Patient Undergoing Multiple Valve Surgery
- Extraction of an Infected Permanent Pacemaker Lead UsingCardiopulmonary Bypass: 2 case reports
- Transvenous Pacemaker Lead Removal in Pacemaker Lead Endocarditis with Large Vegetations: A Report of Two Cases
- A Case of Pacemaker Implantation after Balloon Venoplasty on Innominate Vein Stenosis
