What Is the Ideal Tumor Regression Grading System in Rectal Cancer Patients after Preoperative Chemoradiotherapy?
- Affiliations
-
- 1Department of Pathology, Research Institute and Hospital, National Cancer Center, Goyang, Korea. heejincmd@yahoo.com
- 2Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- 3Division of Colorectal Surgery, Department of Surgery, Seoul National University, Seoul, Korea.
- 4Biometric Research Branch, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- KMID: 2344073
- DOI: http://doi.org/10.4143/crt.2015.254
Abstract
- PURPOSE
Tumor regression grade (TRG) is predictive of therapeutic response in rectal cancer patients after chemoradiotherapy (CRT) followed by curative resection. However, various TRG systems have been suggested, with subjective categorization, resulting in interobserver variability. This study compared the prognostic validity of four different TRG systems in order to identify the most ideal TRG system.
MATERIALS AND METHODS
This study included 933 patients who underwent preoperative CRT and curative resection. Primary tumors alone were graded according to the American Joint Committee on Cancer (AJCC), Dworak, and Ryan TRG systems, and both primary tumors and regional lymph nodes were graded according to a modified Dworak TRG system. The ability of each TRG system to predict recurrence-free survival (RFS) and overall survival (OS) was analyzed using chi-square and C statistics.
RESULTS
All four TRG systems were significantly predictive of both RFS and OS (p < 0.001 each), however none was a better predictor of prognosis than ypStage. Among the four TRGs, the mDworak TRG system was a better predictor of RFS and OS than the AJCC, Dworak, and Ryan TRG systems, and both the chi-square and C statistics were higher for the former, although the differences were not statistically significant. The combination of ypStage and the modified Dworak TRG better predicted RFS and OS than ypStage alone.
CONCLUSION
The modified Dworak TRG system for evaluation of entire tumors including regional lymph nodes is a better predictor of survival than current TRG systems for evaluation of the primary tumor alone.
Figure
-
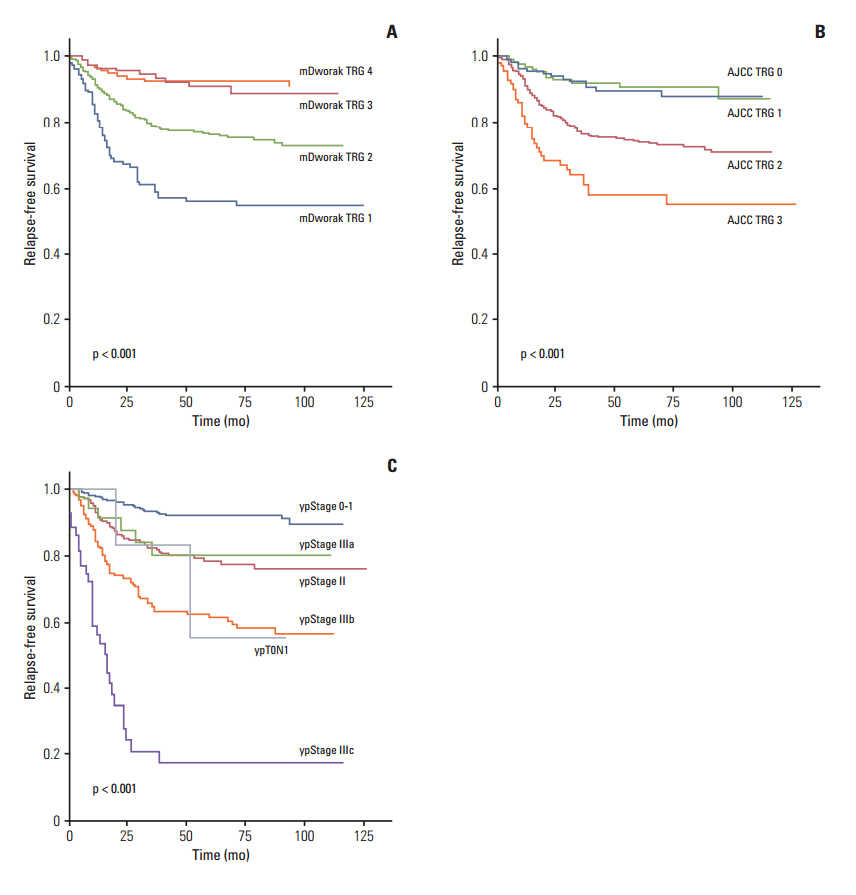
Fig. 1. Relapse-free survival of 933 rectal cancer patients treated with pre-operative chemoradiotherapy followed by surgical resection, according to tumor regression grades (TRG) according to the modified Dworak (mDworak) system (A), which assesses both the primary tumor and regional lymph nodes, the American Joint Committee on Cancer (AJCC) system (B), which assesses the primary tumor alone, and ypStage (C).
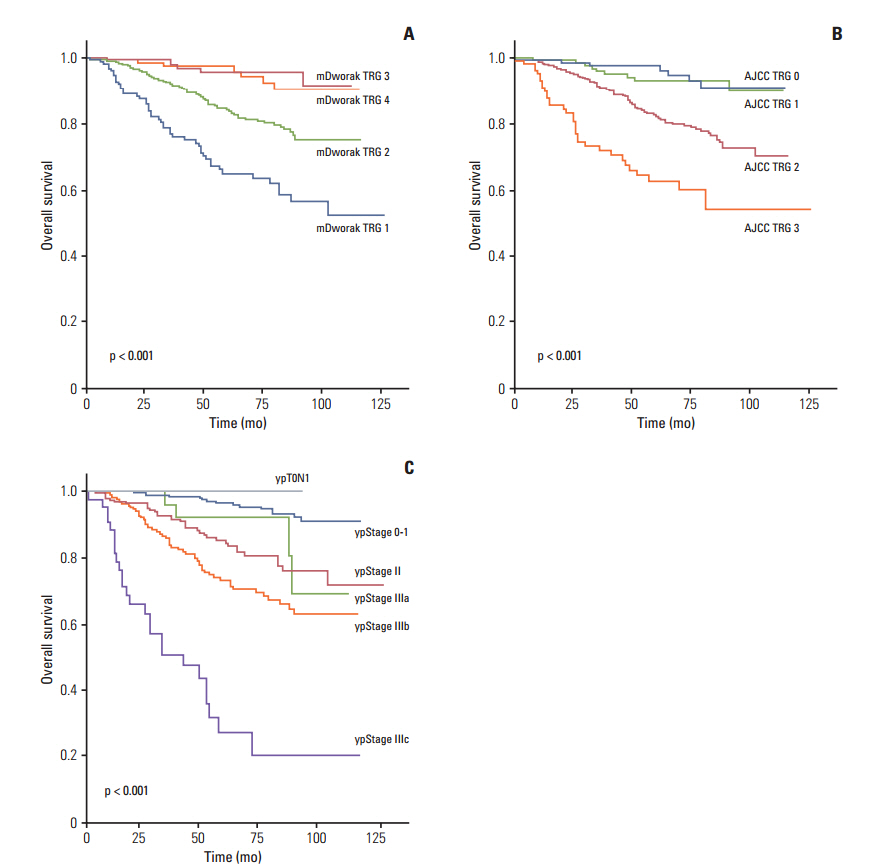
Fig. 2. Overall survival of 933 rectal cancer patients treated with pre-operative chemoradiotherapy followed by surgical resection, according to tumor regression grades (TRG) according to the modified Dworak (mDworak) system (A), which assesses both the primary tumor and regional lymph nodes, the American Joint Committee on Cancer (AJCC) system (B), which assesses the primary tumor alone, and ypStage (C).
Cited by 1 articles
-
Standardized Pathology Report for Colorectal Cancer, 2nd Edition
Baek-hui Kim, Joon Mee Kim, Gyeong Hoon Kang, Hee Jin Chang, Dong Wook Kang, Jung Ho Kim, Jeong Mo Bae, An Na Seo, Ho Sung Park, Yun Kyung Kang, Kyung-Hwa Lee, Mee Yon Cho, In-Gu Do, Hye Seung Lee, Hee Kyung Chang, Do Youn Park, Hyo Jeong Kang, Jin Hee Sohn, Mee Soo Chang, Eun Sun Jung, So-Young Jin, Eunsil Yu, Hye Seung Han, Youn Wha Kim
J Pathol Transl Med. 2020;54(1):1-19. doi: 10.4132/jptm.2019.09.28.
Reference
-
References
1. Quah HM, Chou JF, Gonen M, Shia J, Schrag D, Saltz LB, et al. Pathologic stage is most prognostic of disease-free survival in locally advanced rectal cancer patients after preoperative chemoradiation. Cancer. 2008; 113:57–64.
Article2. Hermanek P, Merkel S, Hohenberger W. Prognosis of rectal carcinoma after multimodal treatment: ypTNM classification and tumor regression grading are essential. Anticancer Res. 2013; 33:559–66.3. Kim DW, Kim DY, Kim TH, Jung KH, Chang HJ, Sohn DK, et al. Is T classification still correlated with lymph node status after preoperative chemoradiotherapy for rectal cancer? Cancer. 2006; 106:1694–700.
Article4. Vecchio FM, Valentini V, Minsky BD, Padula GD, Venkatraman ES, Balducci M, et al. The relationship of pathologic tumor regression grade (TRG) and outcomes after preoperative therapy in rectal cancer. Int J Radiat Oncol Biol Phys. 2005; 62:752–60.
Article5. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A 3rd. AJCC cancer staging manual. 7th ed. New York: Springer-Verlag;2010.6. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Haller DG, et al. AJCC cancer staging manual. 6th ed. New York: Springer-Verlag;2002.7. Fleming ID, Cooper JS, Henson DE, Hutter RV, Kennedy BJ, Murphy GP, et al. AJCC cancer staging manual. 5th ed. Philadelphia, PA: Lippincott-Raven Publishers;1997.8. Lee SD, Kim TH, Kim DY, Baek JY, Kim SY, Chang HJ, et al. Lymph node ratio is an independent prognostic factor in patients with rectal cancer treated with preoperative chemoradiotherapy and curative resection. Eur J Surg Oncol. 2012; 38:478–83.
Article9. Tsai CJ, Crane CH, Skibber JM, Rodriguez-Bigas MA, Chang GJ, Feig BW, et al. Number of lymph nodes examined and prognosis among pathologically lymph node-negative patients after preoperative chemoradiation therapy for rectal adenocarcinoma. Cancer. 2011; 117:3713–22.
Article10. Chetty R, Gill P, Govender D, Bateman A, Chang HJ, Deshpande V, et al. International study group on rectal cancer regression grading: interobserver variability with commonly used regression grading systems. Hum Pathol. 2012; 43:1917–23.
Article11. Ryan R, Gibbons D, Hyland JM, Treanor D, White A, Mulcahy HE, et al. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology. 2005; 47:141–6.
Article12. Dworak O, Keilholz L, Hoffmann A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int J Colorectal Dis. 1997; 12:19–23.
Article13. Mandard AM, Dalibard F, Mandard JC, Marnay J, Henry-Amar M, Petiot JF, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma: clinicopathologic correlations. Cancer. 1994; 73:2680–6.
Article14. Bosman FT, Carneiro F, Hruban RH. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC Press;2010.15. Balakrishnan N, Rao CR. Handbook of statistics: advances in survival analysis. Burlington, MA: Elsevier;2004.16. Rullier A, Laurent C, Capdepont M, Vendrely V, Bioulac-Sage P, Rullier E. Impact of tumor response on survival after radiochemotherapy in locally advanced rectal carcinoma. Am J Surg Pathol. 2010; 34:562–8.
Article17. Suarez J, Vera R, Balen E, Gomez M, Arias F, Lera JM, et al. Pathologic response assessed by Mandard grade is a better prognostic factor than down staging for disease-free survival after preoperative radiochemotherapy for advanced rectal cancer. Colorectal Dis. 2008; 10:563–8.18. Rodel C, Martus P, Papadoupolos T, Fuzesi L, Klimpfinger M, Fietkau R, et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol. 2005; 23:8688–96.19. Rodel C, Liersch T, Becker H, Fietkau R, Hohenberger W, Hothorn T, et al. Preoperative chemoradiotherapy and postoperative chemotherapy with fluorouracil and oxaliplatin versus fluorouracil alone in locally advanced rectal cancer: initial results of the German CAO/ARO/AIO-04 randomised phase 3 trial. Lancet Oncol. 2012; 13:679–87.20. Maas M, Nelemans PJ, Valentini V, Crane CH, Capirci C, Rodel C, et al. Adjuvant chemotherapy in rectal cancer: defining subgroups who may benefit after neoadjuvant chemoradiation and resection: a pooled analysis of 3,313 patients. Int J Cancer. 2015; 137:212–20.
Article21. Yeo SG, Kim DY, Kim TH, Chang HJ, Oh JH, Park W, et al. Pathologic complete response of primary tumor following preoperative chemoradiotherapy for locally advanced rectal cancer: long-term outcomes and prognostic significance of pathologic nodal status (KROG 09-01). Ann Surg. 2010; 252:998–1004.22. Huebner M, Wolff BG, Smyrk TC, Aakre J, Larson DW. Partial pathologic response and nodal status as most significant prognostic factors for advanced rectal cancer treated with preoperative chemoradiotherapy. World J Surg. 2012; 36:675–83.
Article23. Trakarnsanga A, Gonen M, Shia J, Nash GM, Temple LK, Guillem JG, et al. Comparison of tumor regression grade systems for locally advanced rectal cancer after multimodality treatment. J Natl Cancer Inst. 2014; 106:dju248.
Article24. Hong YS, Nam BH, Kim KP, Kim JE, Park SJ, Park YS, et al. Oxaliplatin, fluorouracil, and leucovorin versus fluorouracil and leucovorin as adjuvant chemotherapy for locally advanced rectal cancer after preoperative chemoradiotherapy (ADORE): an open-label, multicentre, phase 2, randomised controlled trial. Lancet Oncol. 2014; 15:1245–53.
Article25. Park SY, Chang HJ, Kim DY, Jung KH, Kim SY, Park JW, et al. Is step section necessary for determination of complete pathological response in rectal cancer patients treated with preoperative chemoradiotherapy? Histopathology. 2011; 59:650–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Significance of Tumor Regression Grade after Preoperative Chemoradiotherapy for Rectal Cancer
- Surgical issues in locally advanced rectal cancer treated by preoperative chemoradiotherapy
- Correlation between tumor regression grade and rectal volume in neoadjuvant concurrent chemoradiotherapy for rectal cancer
- Results of Preoperative Chemoradiotherapy in Low Rectal Cancer
- Clinical Significance of Tumor Regression Grade in Rectal Cancer with Preoperative Chemoradiotherapy
