Embolization of Multiple Systemic Artery to Pulmonary Artery Fistula with Recurrent Hemoptysis
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine and Lung Institute of Medical Research Center, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Radiology, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea. sorock71@snu.ac.kr
Abstract
- Herein, we report a case of multiple systemic arteries to pulmonary artery fistulas without any underlying causes, presenting recurrent hemoptysis. Transcatheter embolization was successfully performed several times on multiple systemic feeding arteries. Multiple systemic arteries to pulmonary fistulas can be a source of uncontrolled bleeding, and embolization may be a reasonable therapeutic option to control the bleeding.
MeSH Terms
Figure
-
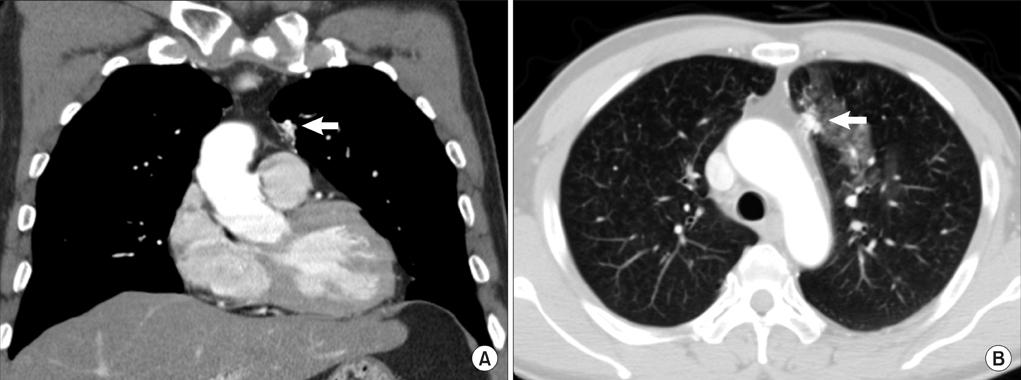
Figure 1 A chest computed tomography image in the mediastinal setting (A) shows that a vascular structure (arrow) abutting on the pericardium is supplied by collateral branches of adjacent vessels. A image in the lung window setting (B) shows about 2.5 cm-sized elongated vascular structure (arrow) in the left upper lobe anterior paramediastinal area. Patch ground-glass-opacities around this are suggestive of aspirated blood.
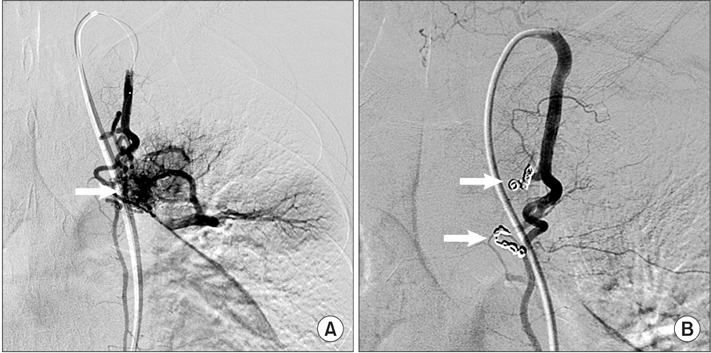
Figure 2 Left internal mammary arteriography (A) shows left internal mammary artery to pulmonary artery fistula (arrow) with 2 feeding vessels. After coil embolization of 2 feeders (arrows), the collateral vessels disappeared (B).
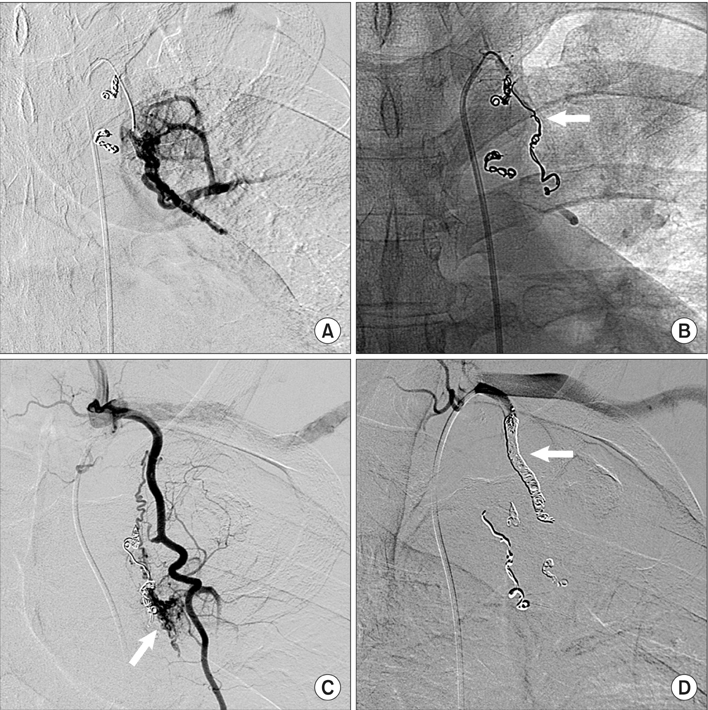
Figure 3 Left subclavian arteriography (A) shows residual systemic artery to pulmonary artery collateral vessels, feed from the proximal portion of left subclavian artery. Coil embolization (arrow) was performed to remove these collateral flows (B). Left internal mammary arteriography (C) shows another collateral vessel from internal mammary artery (arrow). Coil embolization of internal mammary artery (arrow) was performed to prevent hemoptysis (D).
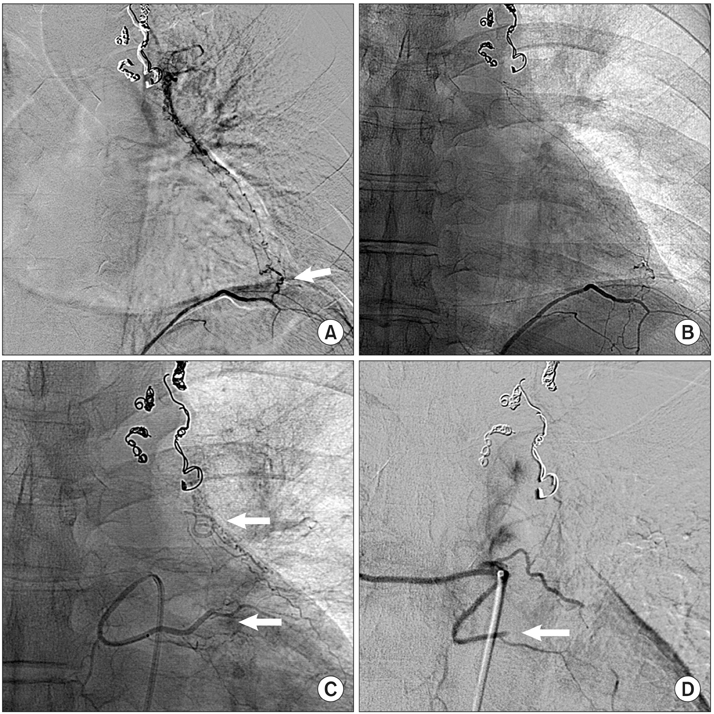
Figure 4 Abdominal aortography (A) shows connections (arrow) of left pericardiacophrenic branch of inferior phrenic artery with pulmonary artery. After embolization with glue, decreased collateral flow was confirmed (B). Left bronchial arteriography (C) reveals additional collateral vessels from left bronchial artery (lower arrow) to pulmonary artery (upper arrow). After embolization for proximal portion of left bronchial artery (arrow) with gel foam, the collateral vessels are not observed (D).
Reference
-
1. Fein AB, Godwin JD, Moore AV, Moran JF, Young WG Jr. Systemic artery-to-pulmonary vascular shunt: a complication of closed-tube thoracostomy. AJR Am J Roentgenol. 1983; 140:917–919.2. Knoepfli HJ, Friedli B. Systemic-to-pulmonary artery fistula following actinomycosis. Chest. 1975; 67:494–496.3. Dunn RP, Wexler L. Systemic-to-pulmonary fistula in intrapulmonary Hodgkin's disease. Chest. 1974; 66:590–594.4. Hirsch M, Maroko I, Gueron M, Goleman L. Systemic-pulmonary arteriovenous fistula of traumatic origin: a case report. Cardiovasc Intervent Radiol. 1983; 6:160–163.5. Yon JR, Ravenel JG. Congenital bronchial artery-pulmonary artery fistula in an adult. J Comput Assist Tomogr. 2010; 34:418–420.6. Hasegawa I, Kobayashi K, Kohda E, Hiramatsu K. Bronchopulmonary arterial anastomosis at the precapillary level in human lung: visualization using CT angiography compared with microangiography of autopsied lung. Acta Radiol. 1999; 40:578–584.7. Yu CH, Chen MR. Clinical investigation of systemic-pulmonary collateral arteries. Pediatr Cardiol. 2008; 29:334–338.8. Geyik S, Yavuz K, Keller FS. Unusual systemic artery to pulmonary artery malformation without evidence of systemic disease, trauma or surgery. Cardiovasc Intervent Radiol. 2006; 29:897–901.9. Ohkura K, Yamashita K, Terada H, Washiyama N, Akuzawa S. Congenital systemic and coronary-to-pulmonary artery fistulas. Ann Thorac Cardiovasc Surg. 2010; 16:203–206.10. Saito T, Matsuda M, Yamaguchi T, Matsuzaki T, Nakagawa S. A case of a traumatic systemic-pulmonary arteriovenous fistula. Jpn Heart J. 1975; 16:196–203.11. Yamada Y, Imamura H, Amamoto Y, Ochi M, Nagano K, Ito M. Congenital internal mammary artery-to-pulmonary artery fistulas: a case report. Heart Vessels. 1987; 3:47–49.12. Huang YK, Lei MH, Lu MS, Tseng CN, Chang JP, Chu JJ. Bilateral coronary-to-pulmonary artery fistulas. Ann Thorac Surg. 2006; 82:1886–1888.13. Itano H, Lee S, Kulick DM, Iannettoni MD, Williams DM, Orringer MB. Nontraumatic chest wall systemic-to-pulmonary artery fistula. Ann Thorac Surg. 2005; 79:e29–e31.14. Dutton JA, Jackson JE, Hughes JM, Whyte MK, Peters AM, Ussov W, et al. Pulmonary arteriovenous malformations: results of treatment with coil embolization in 53 patients. AJR Am J Roentgenol. 1995; 165:1119–1125.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coronary to Bronchial Artery Fistula Causing Massive Hemoptysis in Patients with Longstanding Pulmonary Tuberculosis
- A Case of Pulmonary Artery-bronchial Fistula with Massive Hemoptysis due to Pulmonary Tuberculosis
- Successful Embolization in the Patient with Hemoptysis Due to Right Inferior Phrenic Artery-pulmonary Artery Anastomosis and Pseudoaneurysm
- Arterial Embolization for Management of Hemoptysis
- Endovascular Thrombin Injection for a Pulmonary Artery Pseudoaneurysm: Case Report
