Pediatr Gastroenterol Hepatol Nutr.
2012 Mar;15(1):52-56.
Preoperative Diagnosis of Congenital Esophageal Stenosis Caused by Tracheobronchial Remnants Using Miniprobe Endoscopic Ultrasonography in a Child
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, Dankook University, Cheonan, Korea. pdlks@dankook.ac.kr
Abstract
- Congenital esophageal stenosis (CES) can be classified into three types based on the etiology of stenosis: tracheobronchial remnants (TBRs), fibromuscular hypertrophy (FMH), and membranous diaphragm (MD). It is important to make a differential diagnosis because the therapeutic plan for CES is determined by its etiology. Most cases of FMH and MD can be managed with balloon dilatation, whereas cases of TBRs require resection and anastomosis. Thus, the preoperative distinction of TBRs is critical. Recently miniprobe endoscopic ultrasonography (EUS) with a maximum diameter of 2.5 mm has been useful for distinguishing TBRs from FMH in pediatric patients with CES. EUS shows hyperechoic lesions indicating TBR cartilage. Miniprobe EUS is recommended for choosing the correct therapeutic method for CES. We report a case of CES due to TBRs in which a preoperative diagnosis was made in a child using miniprobe EUS without any difficulties.
MeSH Terms
Figure
-

Fig. 1 Esophageal endoscopy shows a stenotic central lumen at 30 cm distal esophagus from the incisor.

Fig. 2 Esophagography shows a luminal narrowing (arrow) of the distal esophagus with multiple extraluminal filling of barium and dilatation of the proximal esophagus.
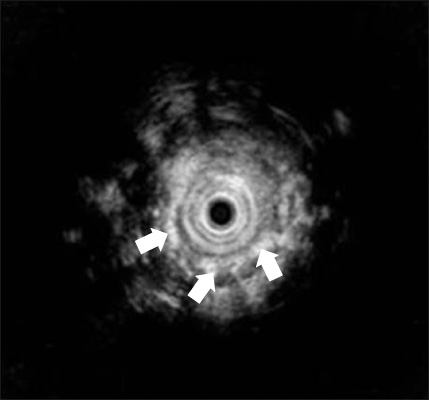
Fig. 3 Endoscopic ultrasonography shows multiple hyperechogenic spots (arrows) spread into muscle layer of a stenotic lesion.
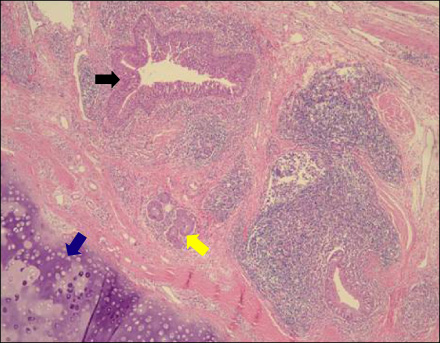
Fig. 4 Histologic picture of the resected specimen shows bronchial cartilage (blue arrow), mucus glands (yellow arrow), and ciliated respiratory epithelium (black arrow) in the esophageal wall (hematoxylin and eosin, ×40).
Reference
-
1. Saito T, Ise K, Kawahara Y, Yamashita M, Shimizu H, Suzuki H, et al. Congenital esophageal stenosis because of tracheobronchial remnant and treated by circular myectomy: a case report. J Pediatr Surg. 2008. 43:583–585.
Article2. Maeda K, Hisamatsu C, Hasegawa T, Tanaka H, Okita Y. Circular myectomy for the treatment of congenital esophageal stenosis owing to tracheobronchial remnant. J Pediatr Surg. 2004. 39:1765–1768.
Article3. Sung GW, Lee SY, Choi YH, Kim KM, Seo JK, Kim IW, et al. Four cases of congenital esophageal stenosis due to tracheobronchial remnants. J Korean Pediatr Soc. 1996. 39:273–279.4. Jang JY, Ko JS, Park KW, Kim IW, Kim WS, Jang JJ, et al. Congenital esophageal stenosis: with special reference to diagnosis and postoperative complications. J Korean Pediatr Soc. 1999. 42:535–544.5. Takamizawa S, Tsugawa C, Mouri N, Satoh S, Kanegawa K, Nishijima E, et al. Congenital esophageal stenosis: therapeutic strategy based on etiology. J Pediatr Surg. 2002. 37:197–201.
Article6. Usui N, Kamata S, Kawahara H, Sawai T, Nakajima K, Soh H, et al. Usefulness of endoscopic ultrasonography in the diagnosis of congenital esophageal stenosis. J Pediatr Surg. 2002. 37:1744–1746.
Article7. Mennigen R, Tuebergen D, Koehler G, Sauerland C, Senninger N, Bruewer M. Endoscopic ultrasound with conventional probe and miniprobe in preoperative staging of esophageal cancer. J Gastrointest Surg. 2008. 12:256–262.
Article8. Nemolato S, De Hertogh G, Van Eyken P, Faa G, Geboes K. Oesophageal tracheobronchial remnants. Gastroenterol Clin Biol. 2008. 32:779–781.
Article9. Amae S, Nio M, Kamiyama T, Ishii T, Yoshida S, Hayashi Y, et al. Clinical characteristics and management of congenital esophageal stenosis: a report on 14 cases. J Pediatr Surg. 2003. 38:565–570.
Article10. Ramesh JC, Ramanujam TM, Jayaram G. Congenital esophageal stenosis: report of three cases, literature review, and a proposed classification. Pediatr Surg Int. 2001. 17:188–192.
Article11. Oh CH, Levine MS, Katzka DA, Rubesin SE, Pinheiro LW, Amygdalos MA, et al. Congenital esophageal stenosis in adults: clinical and radiographic findings in seven patients. AJR Am J Roentgenol. 2001. 176:1179–1182.12. Jeong WS, Jeen YT, Chun HJ, Kim DR, Kwon YD, Lee HS, et al. A case of congenital esophageal stenosis due to tracheobronchial remnants in adult. Korean J Gastrointest Endosc. 2003. 26:21–25.13. Nihoul-Fekete C, De Backer A, Lortat-Jacob S, Pellerin D. Congenital esophageal stenosis: A review of 20 cases. Pediatr Surg Int. 1987. 2:86–92.14. Jones DW, Kunisaki SM, Teitelbaum DH, Spigland NA, Coran AG. Congenital esophageal stenosis: the differential diagnosis and management. Pediatr Surg Int. 2010. 26:547–551.
Article15. Attila T, Adler DG, Hilden K, Faigel DO. EUS in pediatric patients. Gastrointest Endosc. 2009. 70:892–898.
Article16. Bocus P, Realdon S, Eloubeidi MA, Diamantis G, Betalli P, Gamba P, et al. High-frequency miniprobes and 3-dimensional EUS for preoperative evaluation of the etiology of congenital esophageal stenosis in children (with video). Gastrointest Endosc. 2011. 74:204–207.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophageal stenosis due to tracheobronchial remnants: a case report
- Congenital esophageal stenosis due to tracheobronchial remnants
- Four Cases of Congenital Esophageal Stenosis Due to Tracheobronchial Remnants
- Congenital Esophageal Stenosis due to Tracheobronchial Remnants: A case report
- Congenital Esophageal Stenosis in Children: From Etiology to Prognosis
