Effect of Different Sounds on the Treatment Outcome of Tinnitus Retraining Therapy
- Affiliations
-
- 1Department of Otolaryngology-Head & Neck Surgery, Dankook University College of Medicine, Cheonan, Korea.
- 2Department of Otorhinolaryngology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. drmung@naver.com
Abstract
OBJECTIVES
The purpose of this study was to evaluate the therapeutic effect of three different types of sounds on tinnitus patients undergoing tinnitus retraining therapy (TRT).
METHODS
This is a single-institution retrospective study, performed in one tertiary otological referral center. Thirty-eight adults with subjective idiopathic tinnitus who were followed for at least 9 weeks were enrolled. Sound therapy was delivered in 3 different ways: narrowband noise TRT (nTRT); mixed band noise TRT (mTRT); broadband noise TRT (bTRT). Treatment response was measured through validated psychometric questionnaires: Tinnitus Handicap Inventory (THI), visual analog scale (VAS) on annoyance, and numerical description of hours of tinnitus perception (awareness hours).
RESULTS
A total of 38 patients were followed for at least 9 weeks. In nTRT group, all outcome measures including THI, VAS, and the awareness hours, decreased over 9 weeks with no statistical significance. In mTRT group, all outcome measures except for awareness hours significantly improved 9 weeks after the beginning of the treatment. In bTRT group, all outcome measures decreased significantly in 9 weeks. When therapeutic success is defined as improvement in THI 7 or more, bTRT group (77.8%) showed a higher success rate than other groups for 38 patients with the minimum follow-up of 9 weeks.
CONCLUSION
All three sounds can provide relief in patients with annoying tinnitus after TRT. However, there is difference in the therapeutic effect according to sound types. Broadband sound seems to be better than narrowband sound or mixed sound in relieving the patients from tinnitus. Therefore, sound therapy with broadband noise may be more appropriate during TRT, but further evidence is needed for precise conclusion.
Keyword
MeSH Terms
Figure
-
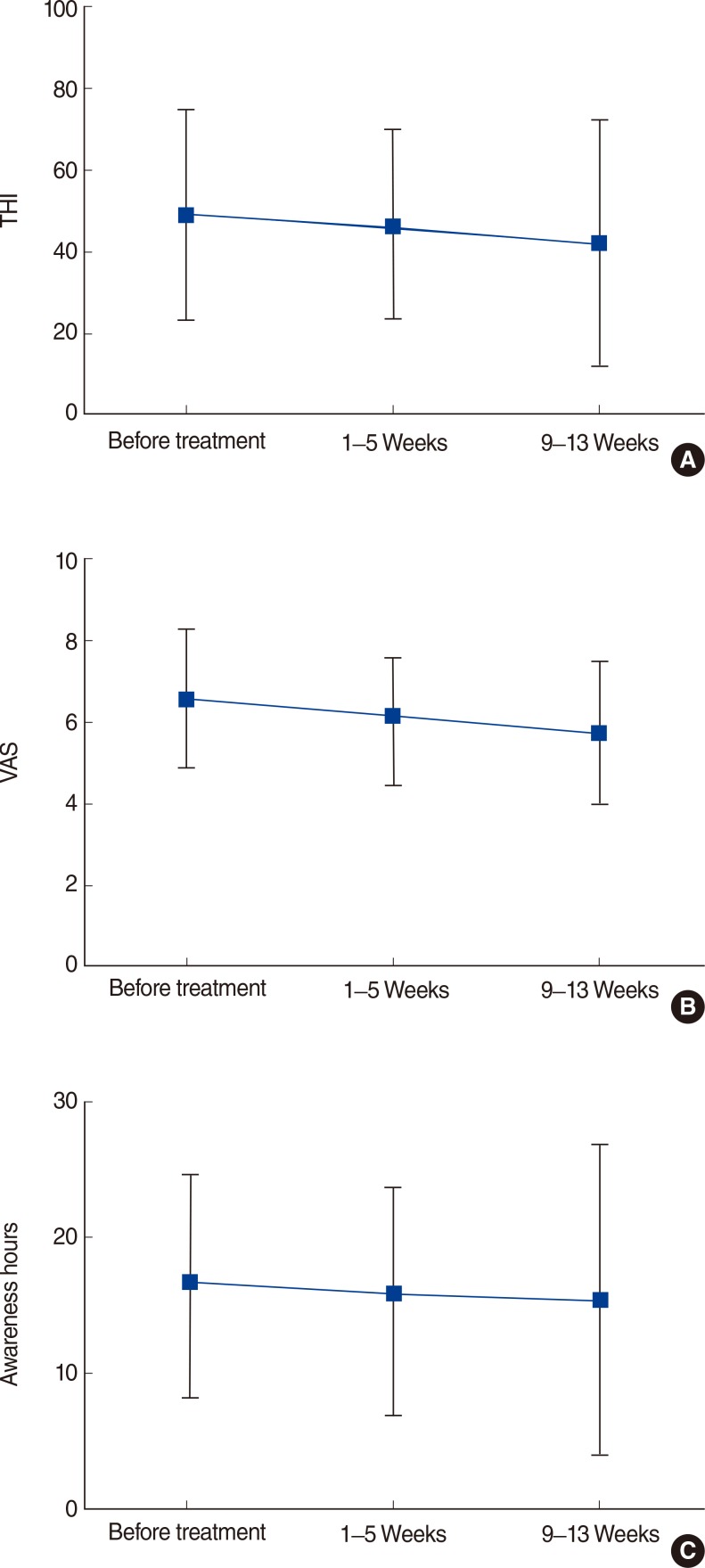
Fig. 1 Mean changes from baseline in questionnaire scores for patients who were treated with narrowband noise tinnitus retraining therapy (nTRT) and followed for more than 9 weeks. All three outcome measures including Tinnitus Handicap Inventory (THI) (A), visual analog scale (VAS) (B), and the awareness hours (C) decreased after 9-13 weeks. THI decreased from 48.25±25.56 to 42.0±29.55, VAS decreased from 6.50±1.60 to 5.63±1.69, and the awareness hours decreased from 16.75±8.41 to 15.13±10.82, respectively.
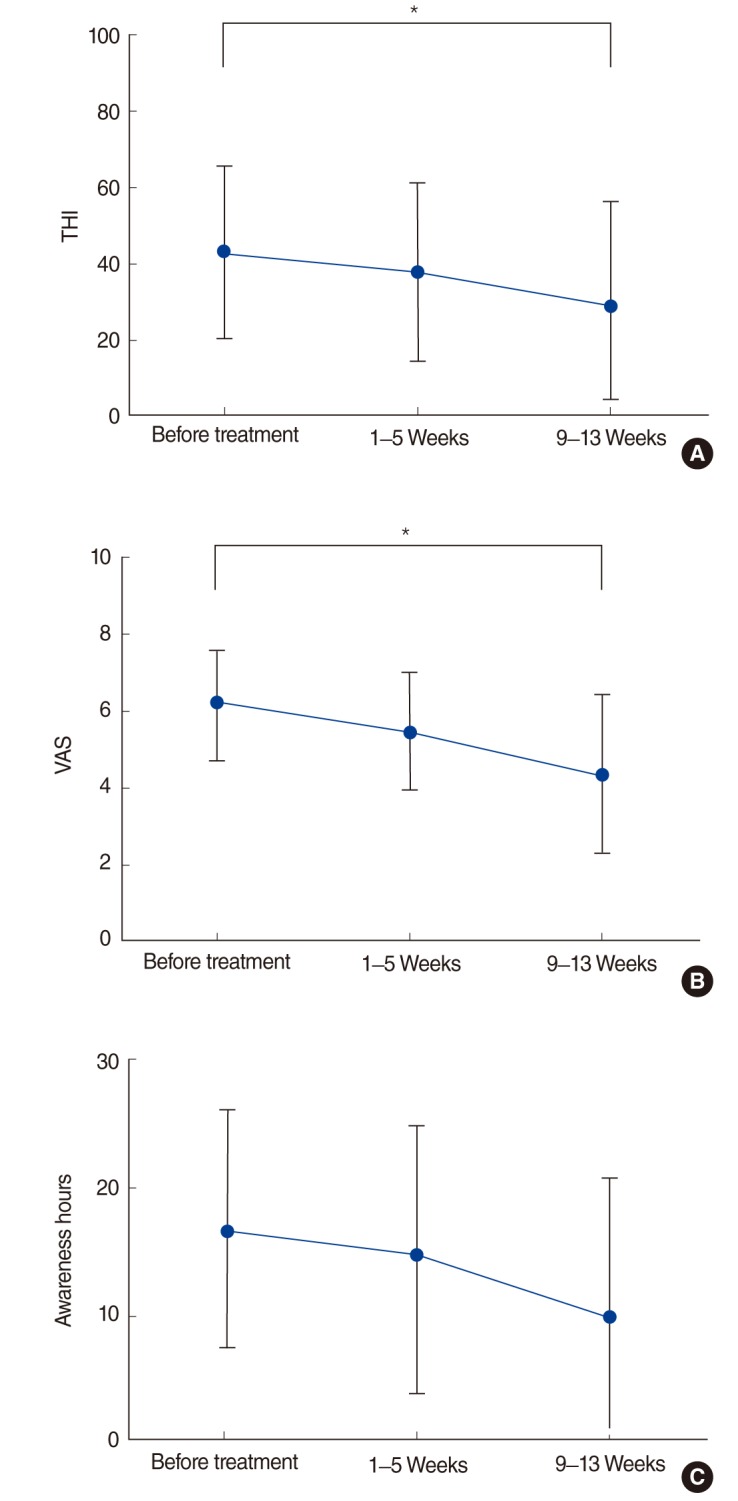
Fig. 2 Mean changes from baseline in questionnaire scores for patients who were treated with mixed noise tinnitus retraining therapy (mTRT) and followed for more than 9 weeks. In mTRT group, Tinnitus Handicap Inventory (THI) (A) and visual analog scale (VAS) (B) significantly decreased for the duration of 9-13 weeks. THI decreased from 42.5±22.27 to 29.0±26.55, VAS decreased from 6.17±1.34 to 4.33±2.06, respectively. Awareness hours (C) decreased from 16.67±9.25 to 9.83±10.94 but it did not reach statistical significance. *P<0.05.
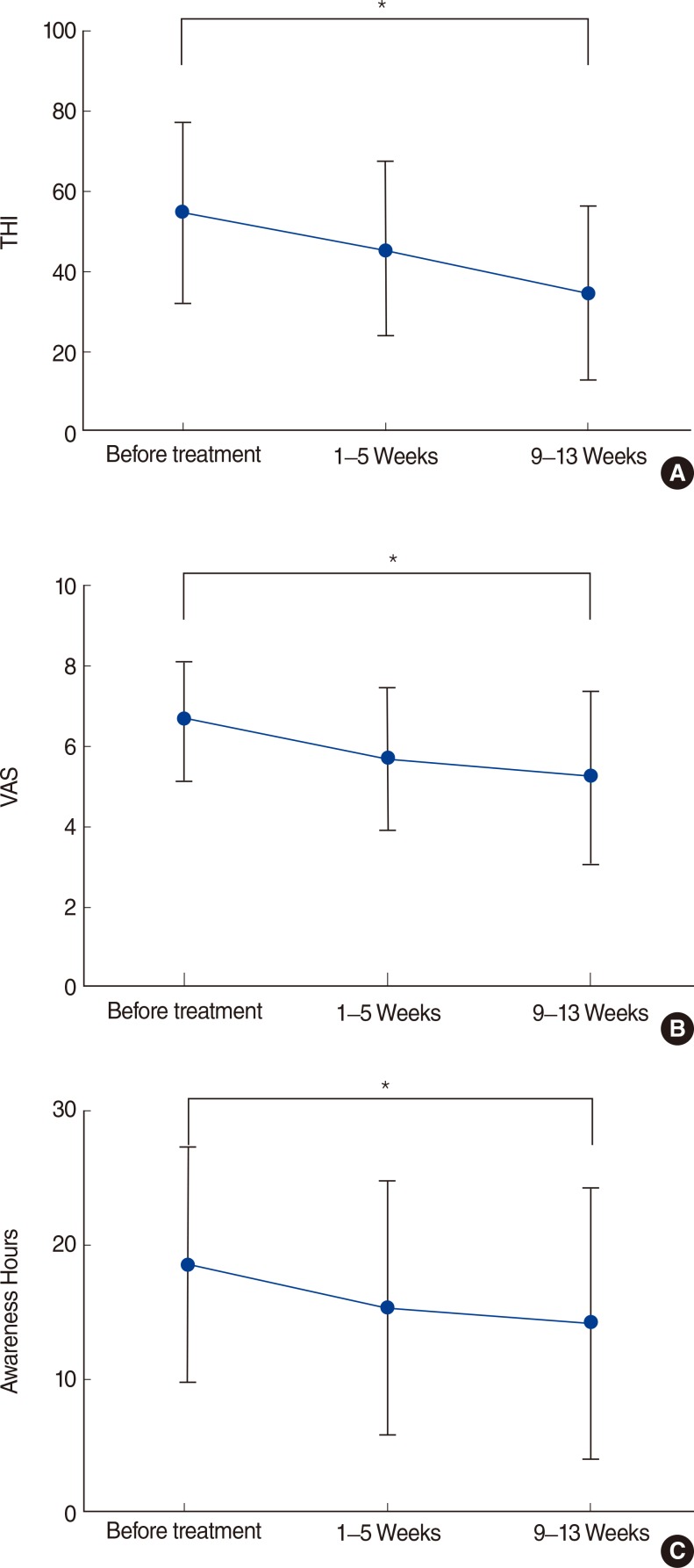
Fig. 3 Mean changes from baseline in questionnaire scores for patients who were treated with broadband noise tinnitus retraining therapy (bTRT) and followed for more than 9 weeks. In bTRT group, all outcome measures showed a statistically significant improvement for 9-13 weeks. Tinnitus Handicap Inventory (THI) (A), visual analog scale (VAS) (B), and the awareness hours (C) decreased significantly from 54.22±22.41 to 35.11±22.44, from 6.50±1.47 to 5.11±2.14, and from 18.17±8.63 to 13.83±10.00, respectively. *P<0.05.
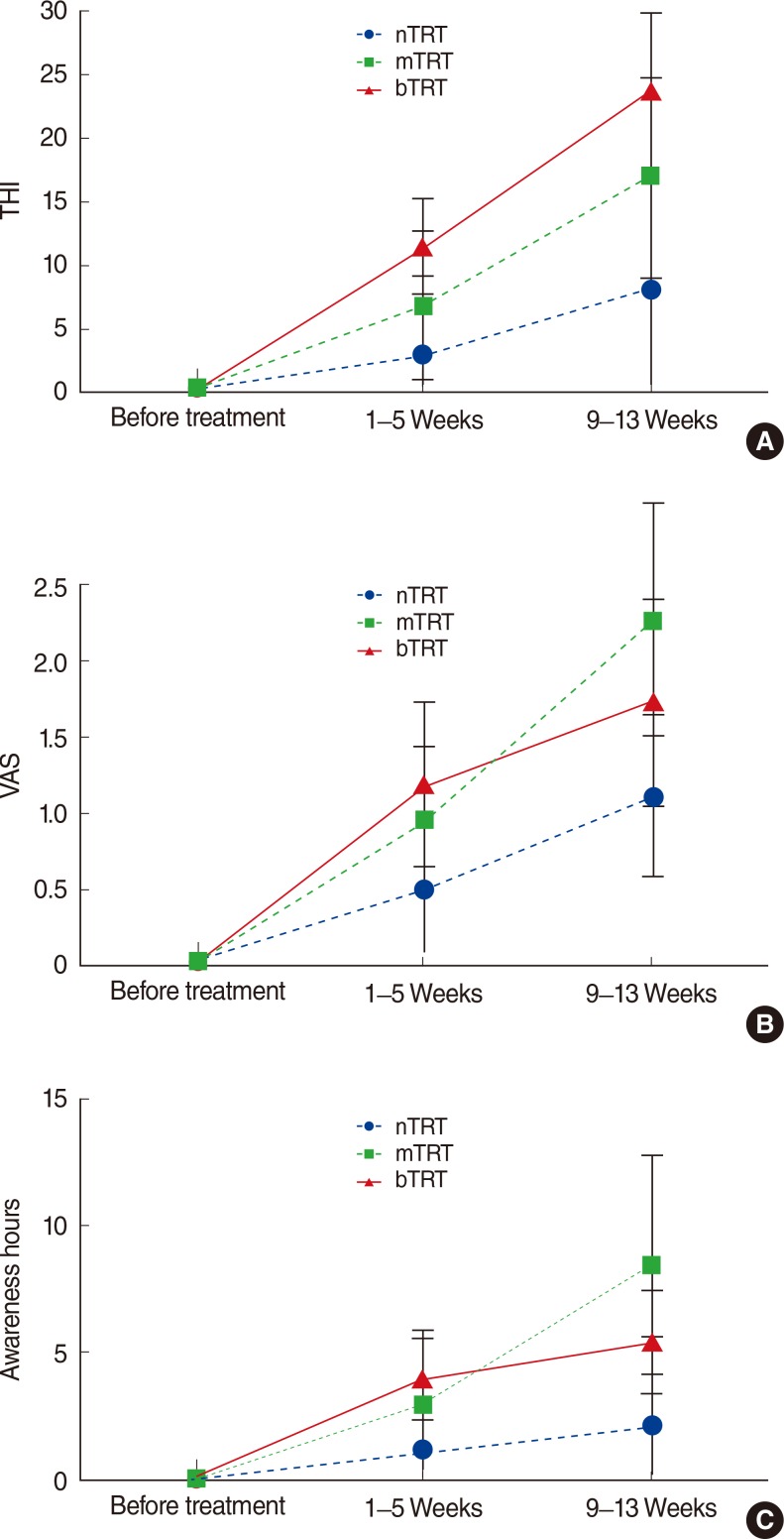
Fig. 4 Improvement in Tinnitus Handicap Inventory (THI), visual analog scale (VAS), and awareness hours for patients who were followed for more than 9 weeks. A gradual improvement over time in THI score was found in all groups. When the change in THI score was compared between groups, broadband noise tinnitus retraining therapy (bTRT) group seemed to show the best results, bTRT showed the poor results, and the effect of mixed noise tinnitus retraining therapy (mTRT) was intermediate (A). VAS also showed a general improvement over time in all three groups. When compared between groups, VAS outcome was comparable between mTRT group and bTRT group, but it was relatively poor in the narrowband noise tinnitus retraining therapy (nTRT) group (B). In terms of awareness hours, a general improvement was shown for the duration of 9-13 weeks. When the change in Awareness Hours was compared between groups, mTRT group and bTRT group showed the comparable improvement, and nTRT group showed the poor result (C). However, all this result did not reach statistical significance.
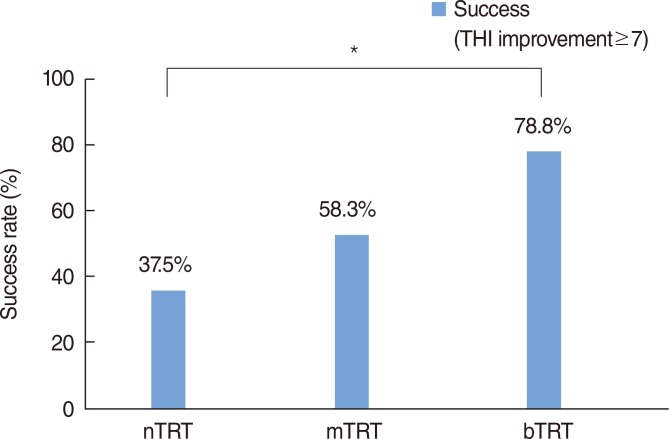
Fig. 5 Comparison of successful treatment rate between groups. The successful treatment rate was 77.8%, 58.3%, and 37.5% for broadband noise tinnitus retraining therapy (bTRT), mixed noise tinnitus retraining therapy (mTRT), and narrowband noise tinnitus retraining therapy (nTRT) group respectively. Sound therapy with broadband noise tended to show better results than that with narrow band noise and mixed noise. THI, Tinnitus Handicap Inventory. *P<0.05.
Reference
-
1. Seidman MD, Jacobson GP. Update on tinnitus. Otolaryngol Clin North Am. 1996; 6. 29(3):455–465. PMID: 8743344.
Article2. Seidman MD, Babu S. Alternative medications and other treatments for tinnitus: facts from fiction. Otolaryngol Clin North Am. 2003; 4. 36(2):359–381. PMID: 12856304.
Article3. Cho IK, Jung JY, Yoo DS, Suh MW. 3-Dimensional reconstruction of the venous system in patients suffering from pulsatile tinnitus. Acta Otolaryngol. 2012; 3. 132(3):285–289. PMID: 22200123.
Article4. Stouffer JL, Tyler RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord. 1990; 8. 55(3):439–453. PMID: 2381186.
Article5. Langguth B, Salvi R, Elgoyhen AB. Emerging pharmacotherapy of tinnitus. Expert Opin Emerg Drugs. 2009; 12. 14(4):687–702. PMID: 19712015.6. Jastreboff PJ, Jastreboff MM. Tinnitus Retraining Therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol. 2000; 3. 11(3):162–177. PMID: 10755812.7. Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy: a different view on tinnitus. ORL J Otorhinolaryngol Relat Spec. 2006; 68(1):23–29. PMID: 16514259.
Article8. Henry JA, Schechter MA, Zaugg TL, Griest S, Jastreboff PJ, Vernon JA, et al. Clinical trial to compare tinnitus masking and tinnitus retraining therapy. Acta Otolaryngol Suppl. 2006; 12. (556):64–69. PMID: 17114146.
Article9. Chung SW, Suh MW. Short term effect of mixed tinnitus retraining therapy. Korean J Otorhinolaryngol-Head Neck Surg. 2011; 10. 54(10):693–698.
Article10. Henry JA, Schechter MA, Nagler SM, Fausti SA. Comparison of tinnitus masking and tinnitus retraining therapy. J Am Acad Audiol. 2002; Nov-Dec. 13(10):559–581. PMID: 12503924.
Article11. Henry JA, Jastreboff MM, Jastreboff PJ, Schechter MA, Fausti SA. Guide to conducting tinnitus retraining therapy initial and follow-up interviews. J Rehabil Res Dev. 2003; Mar-Apr. 40(2):157–177. PMID: 15077641.
Article12. Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol. 1998; 4. 9(2):153–160. PMID: 9564679.13. Jastreboff PJ. Tinnitus retraining therapy. In : Moller AR, editor. Textbook of tinnitus. New York: Springer;2010. p. 575–596.14. Zeman F, Koller M, Figueiredo R, Aazevedo A, Rates M, Coelho C, et al. Tinnitus handicap inventory for evaluating treatment effects: which changes are clinically relevant. Otolaryngol Head Neck Surg. 2011; 8. 145(2):282–287. PMID: 21493265.15. Jastreboff PJ. Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci Res. 1990; 8. 8(4):221–254. PMID: 2175858.
Article16. Jastreboff PJ, Hazell JW. Tinnitus retraining therapy: implementing the neurophysiological model. Cambridge: Cambridge University Press;2004.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short Term Effect of Mixed Tinnitus Retraining Therapy
- Tinnitus Retraining Therapy
- Clinical Implication and Therapeutic Efficacy of Tinnitus Retraining Therapy
- The Effectiveness of the Directive Counseling in Tinnitus Retraining Therapy
- The Effect of Different Counselors on Treatment Outcome of Tinnitus Retraining Therapy
