J Korean Ophthalmol Soc.
2012 Dec;53(12):1737-1741. 10.3341/jkos.2012.53.12.1737.
Effect of the Simultaneous Operation of Levator Resection and Frontalis Suspension for Congenital Ptosis
- Affiliations
-
- 1Department of Ophthalmology, Wonkwang University School of Medicine, Institute of Wonkwang Medical Science, Iksan, Korea. sangduck@wonkwang.ac.kr
- KMID: 2216384
- DOI: http://doi.org/10.3341/jkos.2012.53.12.1737
Abstract
- PURPOSE
To determine retrospectively if a simultaneous frontalis suspension could change the result of undercorrection observed during levator resection in congenital ptosis patients with poor levator functions.
METHODS
Eight eyes in the present study were from 5 infants, 4 infants had congenital ptosis and 1 infant had blepharophimosis. The average age was 3.3 years (range: 1.5 to 6.9 years). If the upper lid margin was not positioned on the superior limbus after performing levator resection under general anesthesia, the height of the upper lid margin was controlled by simultaneous frontalis suspension.
RESULTS
The average follow-up period was 29.8 months. After surgery on both eyes, all 8 cases showed good results and sudden relapse did not occur. Exposed corneal erosion was observed in 6 eyes, but with artificial tears, eye drops, and ointment there were significant improvements within 1 month in all cases. At final examinations, 6 out of 8 eyes showed excellent or good results; undercorrection in 2 eyes was observed and the lateral portion of ptosis in 1 eye was observed as an eye complication.
CONCLUSIONS
If undercorrection caused by levator resection occurs in patients with congenital ptosis, the combination of frontalis suspension surgery may reduce undercorrection and any recurrence that might appear after surgery.
MeSH Terms
Figure
-
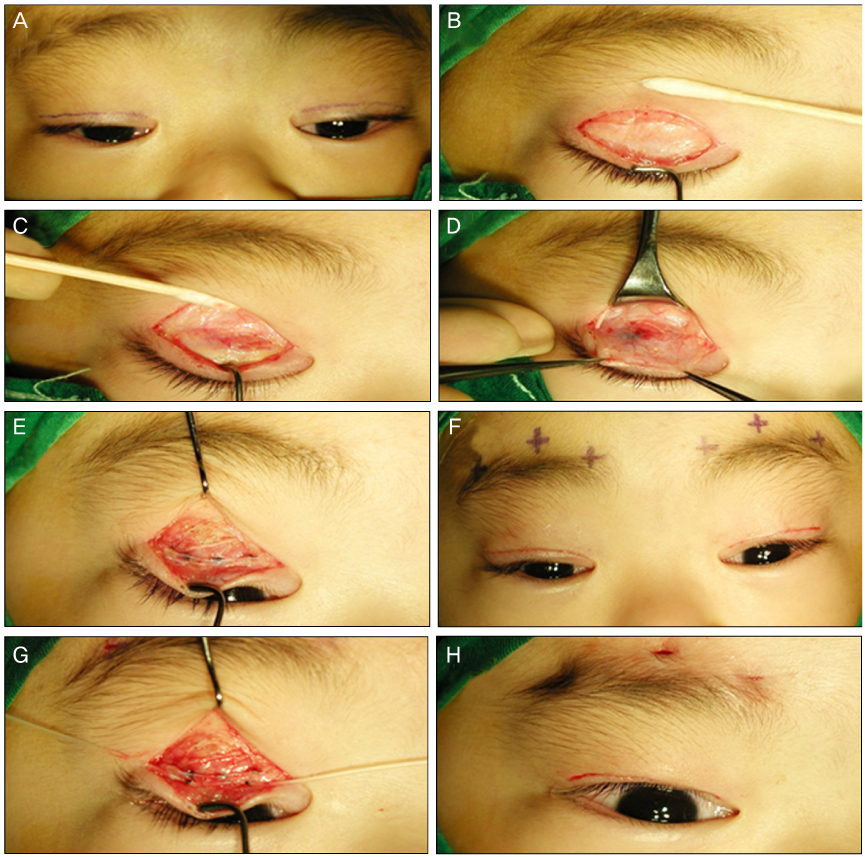
Figure 1 The procedure of the simultaneous levator resection and frontalis suspension for congenital ptosis. The procedure was performed from A to H. The upper lid margin was positioned to superior limbus level.
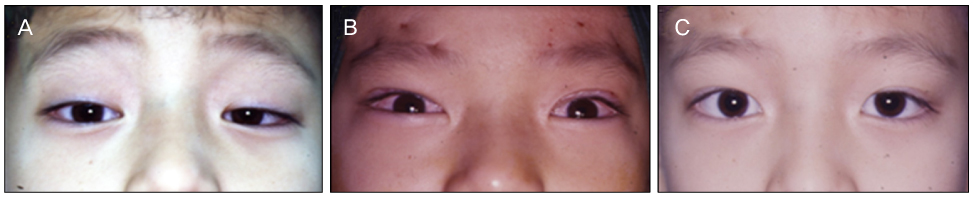
Figure 2 Photograph show excellent results in both eyes after performing our procedure for congenital ptosis. (A) Preoperative photograph. (B) Intraoperative photograph after the last procedure. (C) Postoperative photograph after 13 months.
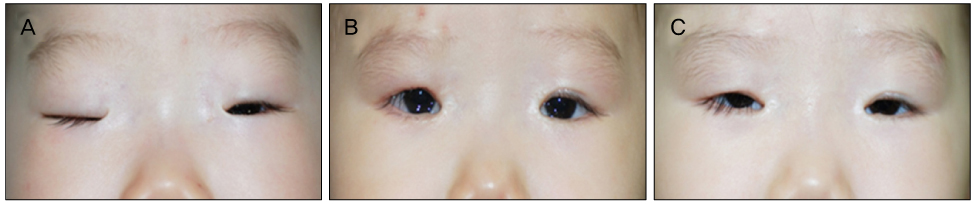
Figure 3 Blepharophimosis infant shows undercorrection after 15 months follow-up. (A) Preoperative photograph. (B) Intraoperative photograph after the last procedure. (C) Postoperative the last follow-up photograph.
Reference
-
1. Wilson ME, Johnson RW. Congenital ptosis. Long-term results of treatment using lyophilized fascia lata for frontalis suspensions. Ophthalmology. 1991. 98:1234–1237.2. Leone CR Jr, Rylander G. A modified silicone frontalis sling for the correction of blepharoptosis. Am J Ophthalmol. 1978. 85:802–805.3. Crawford JS. Recent trends in ptosis surgery. Ann Ophthalmol. 1975. 7:1263–1267.4. Oh JY, Kim C, Chung HK, Khwarg SI. Frontalis sling operation using silicone rod in congenital blepharoptosis patients. J Korean Ophthalmol Soc. 2005. 46:573–580.5. Korean Society of Ophthalmic Plastic and Reconstructive Surgery. Ophthalmic Plastic and Reconstructive Surgery. 2009. 2nd ed. Seoul: Naewae Haksool;128–145.6. Mauriello JA, Wagner RS, Caputo AR, et al. Treatment of congenital ptosis by maximal levator resection. Ophthalmology. 1986. 93:466–469.7. Lee UK, Chung WS. The effect of external levator resection in blepharoptosis with poor levator function. J Korean Ophthalmol Soc. 1998. 39:1062–1068.8. Leibsohn JM. Whitnall's ligament eyelid suspension for severe blepharoptosis. Ophthalmic Surg. 1987. 18:286–287.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes of Anterior Levator Resection and Frontalis Sling in Congenital Ptosis with Poor Levator Function
- Comparison of Frontalis Sling and Levator Resection for Recurrence after Frontalis Sling in Congenital Ptosis
- Use of the Levator Muscle as a Frontalis Sling in Monocular Elevation Deficiency
- COMPARATIVE ANALYSIS BETWEEN LEVATOR RESECTION AND METHODS USING FRONTALIS ACTION 2-4mm OF LEVATOR FUNCTION IN BLEPHAROPTOSIS PATIENTS
- The Frontalis Muscle Transposition in Severe Congenital Ptosis
