Intravitreal Clindamycin Injection for Toxoplasmic Retinochoroiditis
- Affiliations
-
- 1Department of Ophthalmology, Ajou University School of Medicine, Suwon, Korea. dreyesong@naver.com
- KMID: 2215870
- DOI: http://doi.org/10.3341/jkos.2012.53.7.1046
Abstract
- PURPOSE
To present cases of toxoplasmic retinochoroiditis (TRC) treated successfully with intravitreal clindamycin injection.
CASE SUMMARY
(Case 1) A 41-year-old man presented with blurred left eye vision for several months. The patient had a large chorioretinal scar with infiltrations at the boundaries, and fluorescein angiography (FA) showed active retinochoroiditis. Antitoxoplasmosis (antiTX) immunoglobulin G (IgG) was positive, and the patient was started on antiTX medication. Despite several weeks of treatment with maximum doses of antiTx, the TRC progressed and visual acuity worsened. Pars plana vitrectomy (PPV) with intravitreal clindamycin injection (1.0 mg/0.1 ml) was performed, and an additional injection was given 4 weeks later. Six weeks after the second injection, TRC wascompletely resolved with 20/20 vision. (Case 2) A 67-year-old man presented with decreased left eye vision for 1 year. Fundus examinations showed vitreous opacity and epiretinal membranes. The FA revealed retinochoroiditis and the antiTX IgG titer was elevated. The presumed diagnosis was TRC, and oral medications of trimethoprim-sulfamethoxazole, clindamycin, and prednisolone was administered. Inflammation began to improve however, as the patient was not tolerating systemic antiTx medications, an intravitreal injection of clindamycin (1.0 mg/0.1 ml) was administered with PPV. The patientdiscontinued oral medication after surgery, and the inflammation resolved 5 weeks later.
CONCLUSIONS
Intravitreal clindamycin injections may be an additional treatment option for TRC in patients who are unable to tolerate systemic therapy or whose disease progresses despite systemic therapy.
MeSH Terms
Figure
-
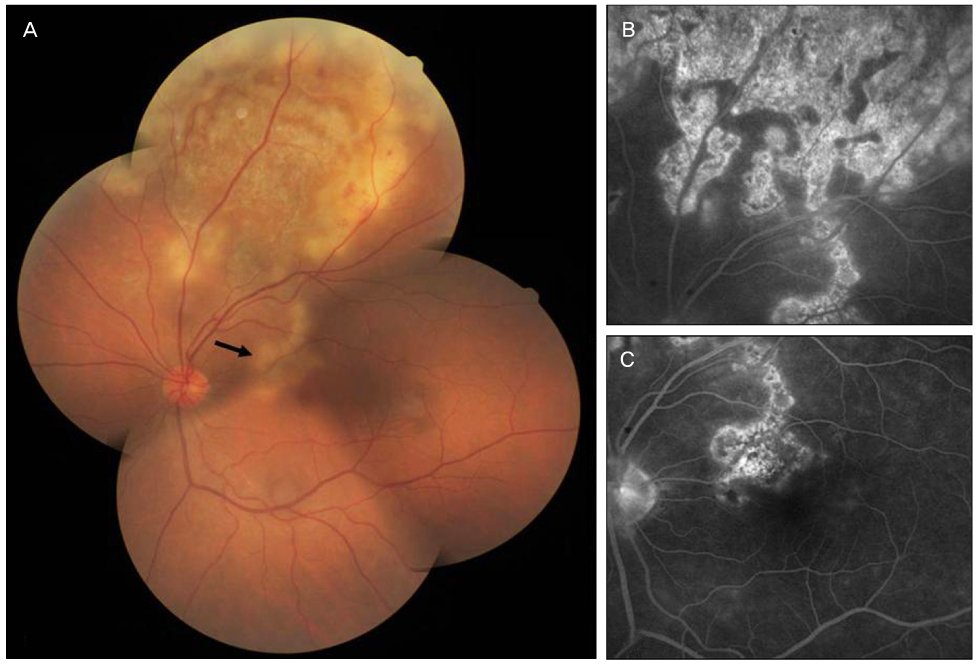
Figure 1 Case 1. Fundus photograph and fluorescein angiographs of the left eye at initial visit. Fundus photograph shows a huge pigmented scar at the superior retina with multiple infiltrations at its margins. The focal retinochoroiditis at the inferior margin of the main lesion (arrow) threatened the fovea (A). Fluorescein angiography reveals staining of the scar and late leakage at the margins (B, C).
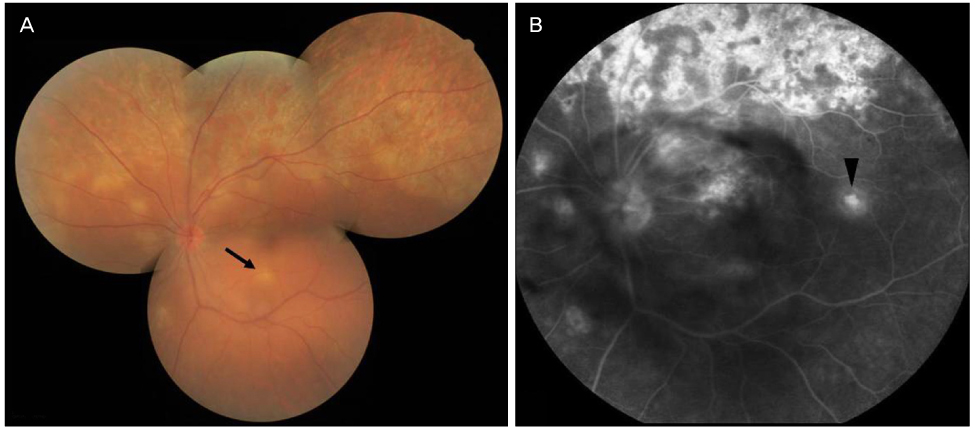
Figure 2 Six weeks after initiation of antitoxoplasmosis medication. Fundus photograph shows that the vitreous opacity was exacerbated and the area of retinochoroiditis had enlarged. A new focal inflammatory lesion(arrow) is noted at the inferior macula (A). In fluorescein angiography, more intense leakage of the lesion is noted with blockage due to increased vitreous opacity. An additional new focal retinitis site (arrowhead) is detected at the temporal macula (B).
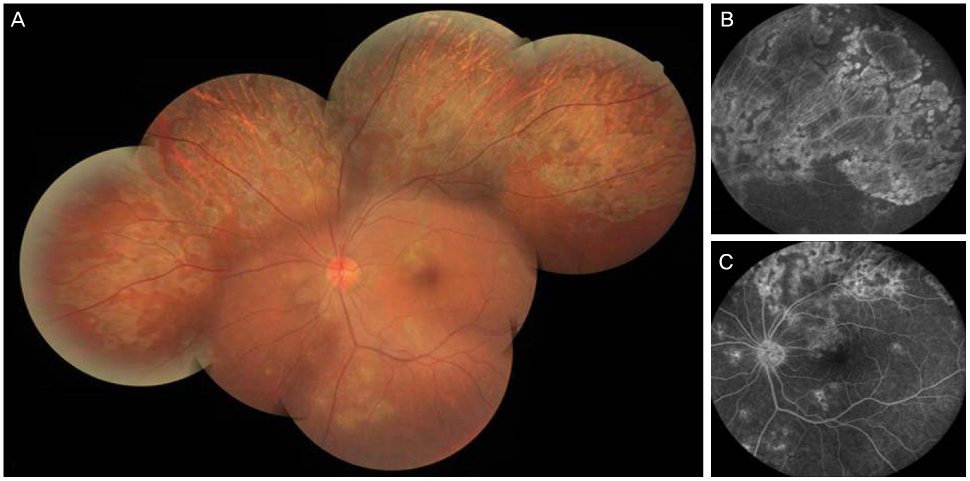
Figure 3 Fundus photograph and fluorescein angiographs at 6 weeks after the second intravitreal clindamycin injection. In fundus photograph, vitreous haze due to vitritis is cleared and all the inflammatory lesions have changed to chorioretinal scars (A). Fluorescein angiography reveals that the previous retinochoroiditis lesions are mainly stained without late leakage (B, C).
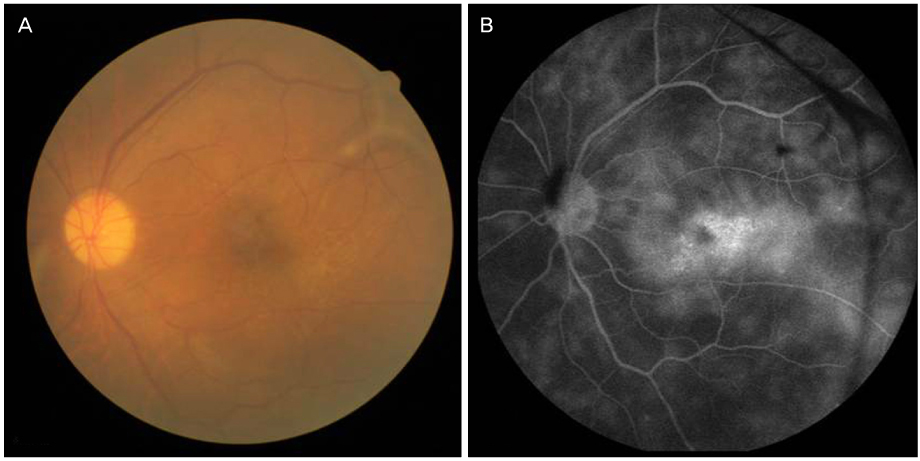
Figure 4 Case 2. Initial fundus photograph of the left eye shows vitreous opacity and a premacular membrane (A). Fluorescein angiography at presentation reveals lateleakage of retinal vasculatures and diffuse retinochoroidal leakage involving the macula (B).
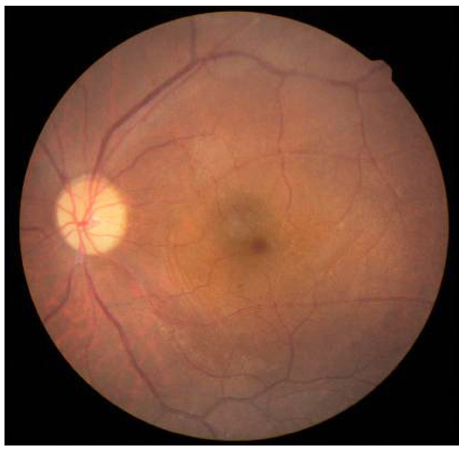
Figure 5 Fundus photograph at 10 weeks after vitrectomy and intravitreal clindamycin injection. Fundus photograph shows clearing of vitreous opacity and no premacular membrane.
Cited by 1 articles
-
Presumed Ocular Toxoplasmosis Presenting as Isolated Unilateral Papillitis
Hye Jin Lee, Sung Gon Kim, Sun Ho Lee, Jin Ho Jeong
J Korean Ophthalmol Soc. 2013;54(9):1463-1468. doi: 10.3341/jkos.2013.54.9.1463.
Reference
-
1. Sobrin L, Kump LI, Foster CS. Intravitreal clindamycin for toxoplasmic retinochoroiditis. Retina. 2007. 27:952–957.2. Soheilian M, Ramezani A, Azimzadeh A, et al. Randomized trial of intravitreal clindamycin and dexamethasone versus pyrimethamine, sulfadiazine, and prednisolone in treatment of ocular toxoplasmosis. Ophthalmology. 2011. 118:134–141.3. Koo L, Young LH. Management of ocular toxoplasmosis. Int Ophthalmol Clin. 2006. 46:183–193.4. Kishore K, Conway MD, Peyman GA. Intravitreal clindamycin and dexamethasone for toxoplasmic retinochoroiditis. Ophthalmic Surg Lasers. 2001. 32:183–192.5. Martinez CE, Zhang D, Conway MD, Peyman GA. Successful management of ocular toxoplasmosis during pregnancy using combined intraocular clindamycin and dexamethasone with systemic sulfadiazine. Int Ophthalmol. 1998-1999. 22:85–88.6. Lasave AF, Díaz-Llopis M, Muccioli C, et al. Intravitreal clindamycin and dexamethasone for zone 1 toxoplasmic retinochoroiditis at twenty-four months. Ophthalmology. 2010. 117:1831–1838.7. Wong R, dell'Omo R, Marino M, et al. Toxoplasma gondii: an atypical presentation of toxoplasma as optic disc swelling and hemispherical retinal vein occlusion treated with intravitreal clindamycin. Int Ophthalmol. 2009. 29:195–198.8. Montoya JG, Parmley S, Liesenfeld O, et al. Use of the polymerase chain reaction for diagnosis of ocular toxoplasmosis. Ophthalmology. 1999. 106:1554–1563.9. Nicholson DH, Wolchok EB. Ocular toxoplasmosis in an adult receiving long-term corticosteroid therapy. Arch Ophthalmol. 1976. 94:248–254.10. Nozik RA. Results of treatment of ocular toxoplasmosis with injectable corticosteroids. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1977. 83:811–818.11. Bovey EH. Usefulness of vitrectomy in the treatment of ocular toxoplasmosis. Int J Med Sci. 2009. 6:139.12. Adan A, Giralt J, Alvarez G, et al. Pars plana vitrectomy for vitreoretinal complications of ocular toxoplasmosis. Eur J Ophthalmol. 2009. 19:1039–1043.13. Papadopoulou DN, Petropoulos IK, Mangioris G, et al. Pars plana vitrectomy in the treatment of severe complicated toxoplasmic retinochoroiditis. Eur J Ophthalmol. 2011. 21:83–88.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fulminant Toxoplasmic Chorioretinitis Following Intravitreal Dexamethasone Implantation
- A Case of Toxoplasmosis Detected in Habitual Aborter
- Two Cases of Ischemic Retinopathy due to Intravitreal Gentamicin Toxicity after Vitrectomy
- Intravitreal and Additional Posterior Subtenon Triamcinolone Injection in Diabetic Macular Edema
- Bilateral Toxoplasma Retinochoroiditis Simulating Cytomegalovirus Retinitis in an Allogeneic Bone Marrow Transplant Patient
