A Case of Non-Arteritic Anterior Ischemic Optic Neuropathy after Bilateral Selective Neck Dissection
- Affiliations
-
- 1Department of Ophthalmology, Ajou University School of Medicine, Suwon, Korea. mingming8@naver.com
- 2Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2215263
- DOI: http://doi.org/10.3341/jkos.2012.53.1.180
Abstract
- PURPOSE
To report a case of non-arteritic anterior ischemic optic neuropathy after bilateral selective neck dissection.
CASE SUMMARY
A 48-year-old man presented with a visual field defect in his right eye 11 days after bilateral selective neck dissection. His corrected visual acuity in the right eye was 20/20; fundus photographs revealed a segmental optic disc swelling in the superior half of the right eye, and the Humphrey visual field test showed an inferior altitudinal defect in the right eye, corresponding to the disc swelling. The fluorescein angiography revealed a delayed filling on the superior half of the optic disc in the right eye. The diagnosis was non-arteritic anterior ischemic optic neuropathy. Orbital and brain MRIs showed an increase in caliber of the right optic nerve, but no other mass or enhanced lesion was noted. After 3 months, the patient's visual acuity and visual field were maintained, but segmental atrophy developed on the superior half of the right optic disc.
CONCLUSIONS
With the risk factors of ischemic optic neuropathy, the possibility of postoperative visual impairment or field defect should be considered after a selective head and neck surgery.
MeSH Terms
Figure
-

Figure 1 Cervical lymph node: division of cervical neck lymph nodes by levels. Level I= submental and submandibular group; level II= upper jugular group; level III = middle jugular group; level IV = lower jugular group; level V = posterior triangular group; level VI = anterior compartment group; level VII = superior mediastinal group.
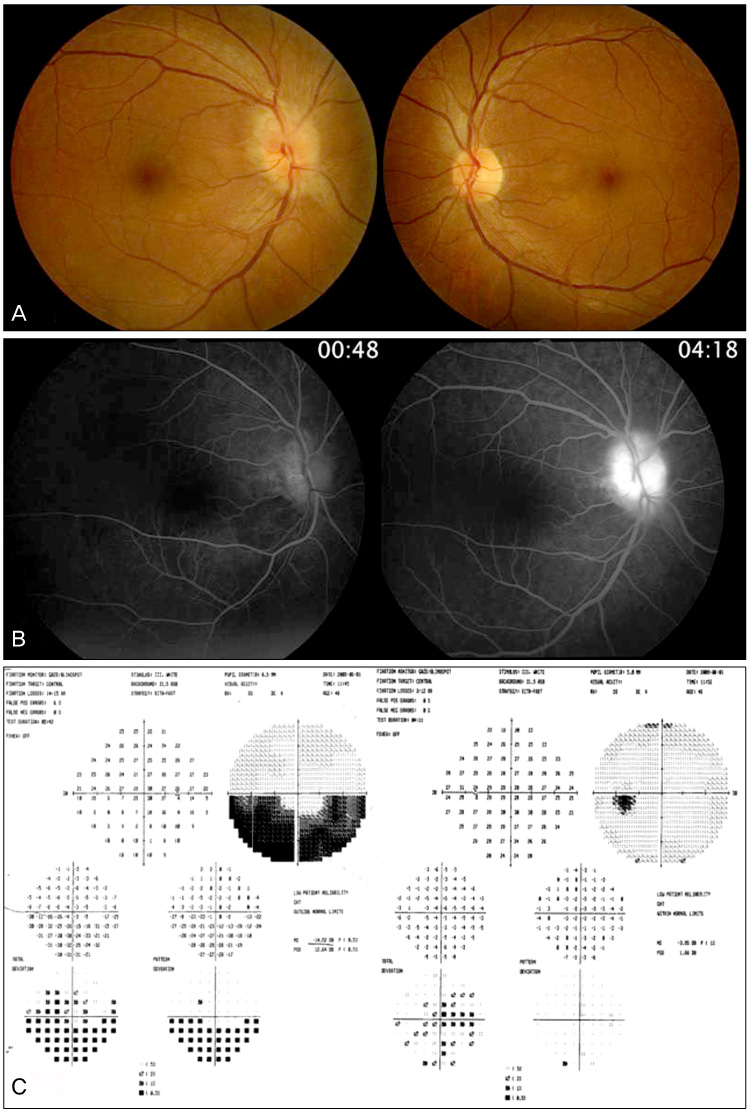
Figure 2 (A) Fundus photographs show an optic disc swelling at the superior half of the right eye. (B) Fluorescein angiography shows a delayed filling and leakage on the superior half of the optic disc in the right eye. (C) Humphrey visual field test reveals inferior altitudinal field defect of the right eye, respecting the horizontal meridian.
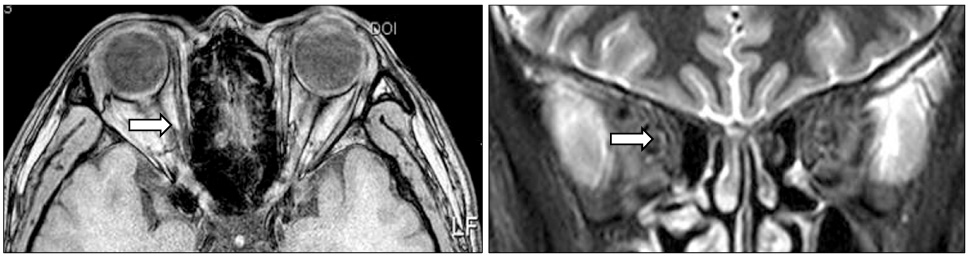
Figure 3 Axial and coronal view of orbital MRI (Gd enhanced) show mild increase in caliber of the right optic nerve (indicated by the white arrows). No mass lesion or abnormal enhancement is observed in the brain and optic nerve.
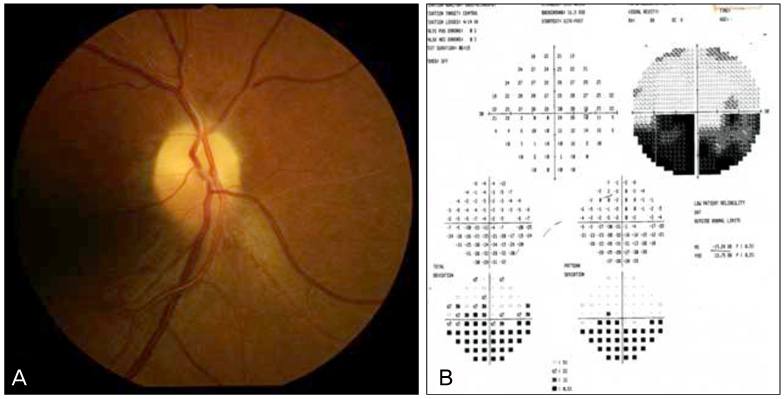
Figure 4 Three months after surgery, segmental atrophy is observed on the superior half of the right optic disc (A). There is no change in the inferior altitudinal field defect of the right eye (B).
Cited by 1 articles
-
Bilateral Anterior Ischemic Optic Neuropathy after Gastrointestinal Bleeding
Jae Sang Ko, Gyu Ah Kim, Joo Youn Shin, Suk Ho Byeon
J Korean Ophthalmol Soc. 2014;55(1):161-166. doi: 10.3341/jkos.2014.55.1.161.
Reference
-
1. Aydin O, Memisoglu I, Ozturk M, Altintas O. Anterior ischemic optic neuropathy after unilateral radical neck dissection: case report and review. Auris Nasus Larynx. 2008. 35:308–312.2. Kim DH, Hwang JM. Risk factors for Korean patients with anterior ischemic optic neuropathy. J Korean Ophthalmol Soc. 2007. 48:1527–1531.3. Suárez-Fernández MJ, Clariana-Martín A, Mencía-Gutiérrez E, et al. Bilateral anterior ischemic optic neuropathy after bilateral neck dissection. Clin Ophthalmol. 2010. 4:95–100.4. Fenton S, Fenton JE, Browne M, et al. Ischemic optic neuropathy following bilateral neck dissection. J Laryngol Otol. 2001. 115:158–160.5. Newman NJ. Perioperative visual loss after nonocular surgeries. Am J Ophthalmol. 2008. 145:604–610.6. Götte K, Riedel F, Knorz MC, Hörmann K. Delayed anterior ischemic optic neuropathy after neck dissection. Arch Otolaryngol Head Neck Surg. 2000. 126:220–223.7. Strome SE, Hill JS, Burnstine MA, et al. Anterior ischemic optic neuropathy following neck dissection. Head Neck. 1997. 19:148–152.8. Wilson JF, Freeman SB, Breene DP. Anterior ischemic optic neuropathy causing blindness in the head and neck surgery patient. Arch Otolaryngol Head Neck Surg. 1991. 117:1304–1306.9. Bell RA, Waggoner PM, Boyd WM, et al. Clinical grading of relative afferent pupillary defects. Arch Ophthalmol. 1993. 111:938–942.10. Park WC, Chang BL. Clinical features of anterior ischemic optic neuropathy. J Korean Ophthalmol Soc. 2003. 44:144–149.11. Boghen DR, Glaser JS. Ischaemic optic neuropathy. The clinical profile and history. Brain. 1975. 98:689–708.12. Arnold AC, Hepler RS. Natural history of nonarteritic anterior ischemic optic neuropathy. J Neuroophthalmol. 1994. 14:66–69.13. Jun BK, Kim DS, Ko MK. Clinical features in anterior ischemic optic neuropathy. J Korean Ophthalmol Soc. 1999. 40:3460–3467.14. Mathews MK. Nonarteritic anterior ischemic optic neuropathy. Curr Opin Ophthalmol. 2005. 16:341–345.15. Kerr NM, Chew SS, Danesh-Meyer HV. Non-arteritic anterior ischaemic optic neuropathy: a review and update. J Clin Neurosci. 2009. 16:994–1000.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Anterior Ischemic Optic Neuropethy
- A Case of Subtype Giant Cell Arteritis Without Symptoms of Arteritic Anterior Ischemic Optic Neuropathy
- Subretinal Fluid Collection in Patient With Non-Arteritic Anterior Ischemic Optic Neuropathy: A Case Report
- Temporal Arteritis with Diagnostic Brain Magnetic Resonance Imaging
- A Case of Acute Nonarteritic Anterior Ischemic Optic Neuropathy in Patient on Hemodialysis
