Risk of Vertebral Artery Injury: A Comparison between C2 Subarticular Segmental and C1-2 Transarticular Screws
- Affiliations
-
- 1Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. ortho@hananet.net
- KMID: 2186418
- DOI: http://doi.org/10.4055/jkoa.2008.43.5.572
Abstract
-
PURPOSE: We compared the risk of vertebral artery injury associated with the insertion of C1-2 transarticular screws and C2 subarticular segmental screws using a computer simulation of computed tomography (CT) scans.
MATERIALS AND METHODS
We simulated the placement of C1-2 transarticular screws and C2 subarticular segmental screws using 1-mm interval CT scan images in 166 patients, along with simulation software. We then determined the incidence of violation of the C2 vertebral artery groove. The same determination was performed for high-riding vertebral arteries found among those patients.
RESULTS
Among the 332 C2 vertebral artery grooves (166 patients), C1-2 transarticular screws violated the groove in 33 (9.9%) instances, while C2 subarticular segmental screws violated the groove in 19 (5.7%) instances. The difference in incidence between the two screw types was statistically significant (p=0.001, McNemar test). In the 48 high-riding vertebral arteries, C1-2 transarticular screws led to violation of the C2 vertebral artery groove in 30 (62.5%) instances, while C2 subarticular segmental screws led to violation of the groove in 18 (37.5%) instances. The difference in incidence between the two screw types was statistically significant (p=0.002, McNemar test).
CONCLUSION
Use of C2 subarticular segmental screws is associated with a lower risk of vertebral artery injury than is the use of C1-2 transarticular screws, even for high-riding vertebral arteries.
Figure
-
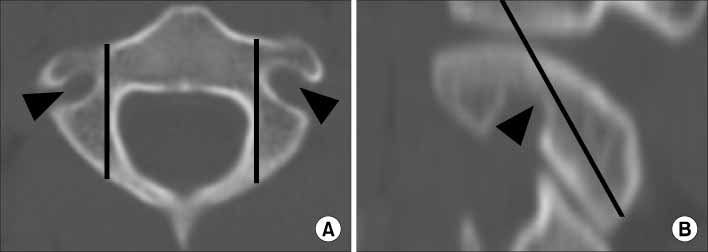
Fig. 1 Vertebral artery grooves (arrowheads) are shown in axial (A) and sagittal (B) CT scan images along with the trajectories of the transarticular screws (black lines). Vertebral artery grooves are located lateral (A) and anterior (B) to the transarticular screws.
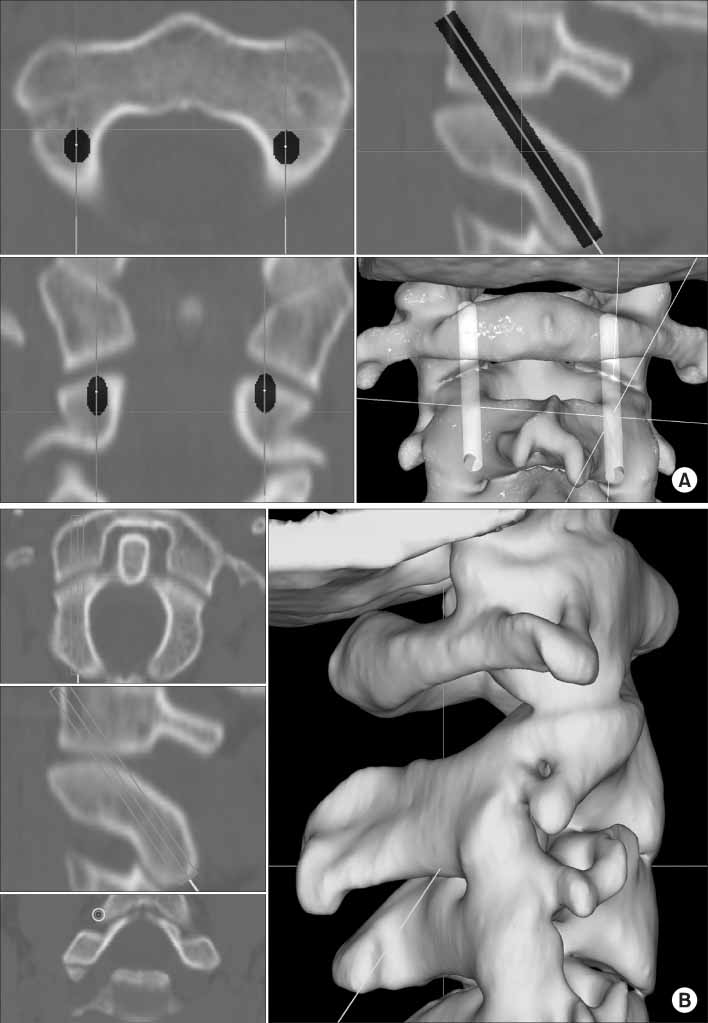
Fig. 2 The trajectory of the transarticular screw is shown. The entry point is set at 3 mm cranial to the caudal edge of the C2 inferior articular process (A) and as medial as possible without penetrating the lateral wall of the spinal canal (B). The upward angulation is afforded as much as possible while maintaining the screw within the posterior boundary of the superior articular surface of C2.
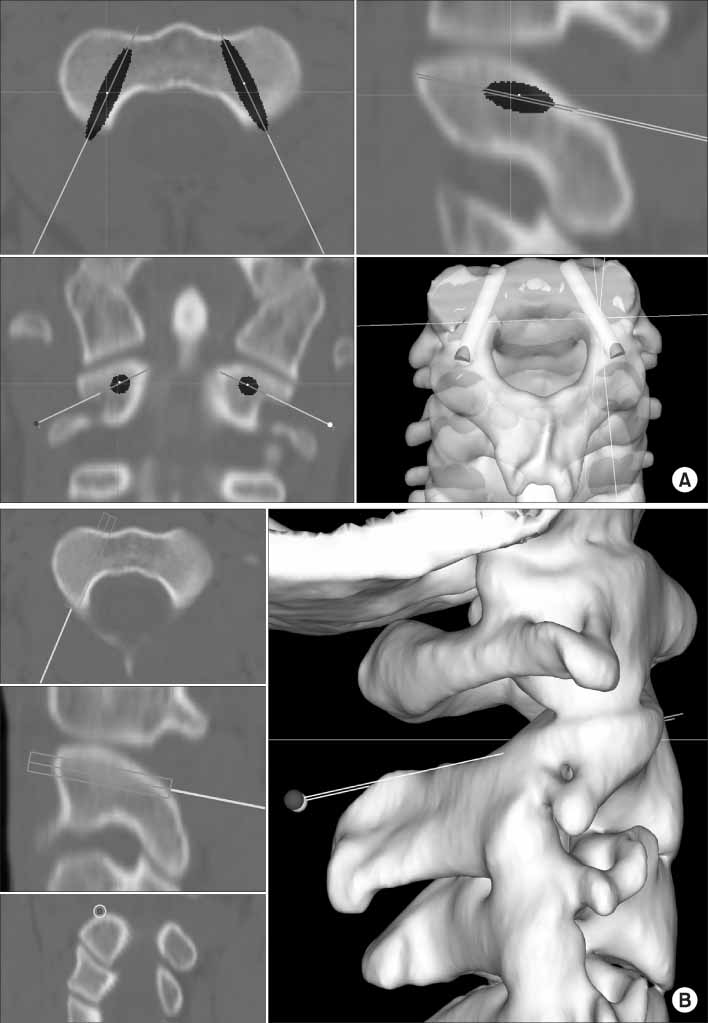
Fig. 3 The trajectory of the subarticular segmental screw is shown. Medial angulation is the same as that of the pedicle on the axial CT images (A). The screw is angled toward the antero-superior end of the superior articular process of C2 in lateral fluoroscopy. The entry point is 3 mm caudal to the posterior aspect of the superior articular surface, and the screw is inserted close to the superomedial border of the superior articular process (B).
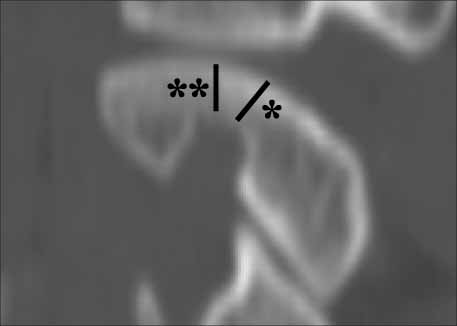
Fig. 4 The two heights that were used to distinguish the high-riding vertebral artery are shown. It is defined by an isthmus height (*) less than 5 mm and/or an internal height (**) less than 2 mm.
Reference
-
1. Bloch O, Holly LT, Park J, Obasi C, Kim K, Johnson JP. Effect of frameless stereotaxy on the accuracy of C1-2 transarticular screw placement. J Neurosurg. 2001. 95:Supple 1. S74–S79.
Article2. Farey ID, Nadkarni S, Smith N. Modified Gallie technique versus transarticular screw fixation in C1-C2 fusion. Clin Orthop Relat Res. 1999. 359:126–135.
Article3. Goel A, Desai KI, Muzumdar DP. Atlantoaxial fixation using plate and screw method: a report of 160 treated patients. Neurosurgery. 2002. 51:1351–1357.
Article4. Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26:2467–2471.
Article5. Igarashi T, Kikuchi S, Sato K, Kayama S, Otani K. Anatomic study of the axis for surgical planning of transarticular screw fixation. Clin Orthop Relat Res. 2003. 408:162–166.
Article6. Jeanneret B. Posterior transarticular screw fixation of C1-C2. Tech Orthop. 1994. 9:49–59.
Article7. Madawi AA, Casey AT, Solanki GA, Tuite G, Veres R, Crockard HA. Radiological and anatomical evaluation of the atlantoaxial transarticular screw fixation technique. J Neurosurg. 1997. 86:961–968.
Article8. Mandel IM, Kambach BJ, Petersilge CA, Johnstone B, Yoo JU. Morphologic considerations of C2 isthmus dimensions for the placement of transarticular screws. Spine. 2000. 25:1542–1547.
Article9. Neo M, Matsushita M, Iwashita Y, Yasuda T, Sakamoto T, Nakamura T. Atlantoaxial transarticular screw fixation for a high-riding vertebral artery. Spine. 2003. 28:666–670.
Article10. Neo M, Matsushita M, Yasuda T, Sakamoto T, Nakamura T. Use of an aiming device in posterior atlantoaxial transarticular screw fixation. Technical note. J Neurosurg. 2002. 97:Suppl 1. S123–S127.11. Neo M, Sakamoto T, Fujibayashi S, Nakamura T. A safe screw trajectory for atlantoaxial transarticular fixation achieved using an aiming device. Spine. 2005. 30:E236–E242.
Article12. Paramore CG, Dickman CA, Sonntag VK. The anatomical suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg. 1996. 85:221–224.
Article13. Prabhu VC, France JC, Voelker JL, Zoarski GH. Vertebral artery pseudoaneurysm complicating posterior C1-2 transarticular screw fixation: case report. Surg Neurol. 2001. 55:29–33.
Article14. Resnick DK, Lapsiwala S, Trost GR. Anatomic suitability of the C1-C2 complex for pedicle screw fixation. Spine. 2002. 27:1494–1498.
Article15. Solanki GA, Crockard HA. Peroperative determination of safe superior transarticular screw trajectory through the lateral mass. Spine. 1999. 24:1477–1482.
Article16. Wright NM, Lauryssen C. Vertebral artery injury in C1-2 transarticular screw fixation: results of a survey of the AANS/CNS section on disorders of the spine and peripheral nerves. American Association of Neurological Surgeons/Congress of Neurological Surgeons. J Neurosurg. 1998. 88:634–640.17. Yeom JS, Won JH, Park SK, et al. The subarticular screw: a new trajectory for the C2 screw. J Kor Soc Spine Surg. 2006. 13:75–80.
Article18. Yoshida M, Neo M, Fujibayashi S, Nakamura T. Comparison of the anatomical risk for vertebral artery injury associated with the C2-pedicle screw and atlantoaxial transarticular screw. Spine. 2006. 31:E513–E517.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atlantoaxial Fixation using C2 Subarticular Screws and C1 Lateral Mass Screws : A Technical Report
- Old Atlantoaxial Rotary Subluxation Associated with High-riding Vertebral Arteries: Arthrodesis Using C1 Lateral Mass Screws and C2 Laminar Screws: A Case Report
- Posterior Atlantoaxial Fixation with a Combination of Pedicle Screws and a Laminar Screw in the Axis for a Unilateral High-riding Vertebral Artery
- Atlantoaxial Stabilization Using C1 and C2 Laminar Screw Fixation
- The Results and Complications of the C1-C2 Transarticular Screw Fixation Methods
