A Case of Scrub Typhus in Summer Presenting as Atypical Pneumonia
- Affiliations
-
- 1Department of Internal Medicine, Inha University College of Medicine, Inchon, Korea. mhchungid@paran.com
- 2Clinical Research Center, Inha University College of Medicine, Inchon, Korea.
- 3Department of Microbiology, Inha University College of Medicine, Inchon, Korea.
- KMID: 2170241
- DOI: http://doi.org/10.3947/ic.2008.40.4.241
Abstract
- Scrub typhus usually occurs in October and November in Korea. Its typical clinical manifestations are fever, rash, eschar, and lymphadenopathies. Pneumonitis may occur, however, it occurs as a complication at the late phase of scrub typhus, when it is inappropriately treated. We encountered a case of pneumonitis that was an initial manifestation of scrub typhus which was confirmed by rickettsial culture, positive seroconversion, and polymerase chain reaction. The case was a 16-year-old high school adolescent who presented with fever and headache that lasted for 1 day in July, 2007. He denied of any outdoor activities. A chest radiograph showed patchy infiltrates in the left lower lung, which improved with the administration of cefotaxime and azithromycin for empirical treatment of community-acquired pneumonia. Blood taken on the second febrile day showed a positive culture for Orientia tsutsugamushi and was also positive for O. tsutsugamushi DNA polymerase chain reaction. Immunofluorescent antibody (IFA) test for O. tsutsugamushi showed that the initial antibody was negative, but convalescent serum tested positive with an antibody titer of 1:80. IFA for Coxiella burnetii showed false positive results; the initial IgM and IgG titers were 1:128 and 1:256, respectively, and the IgM and IgG titers in convalescent serum were 1:128 and 1:128, respectively.
Keyword
MeSH Terms
Figure
-

Figure 1 The chest PA on admission shows infiltrates in the left lower lung field.
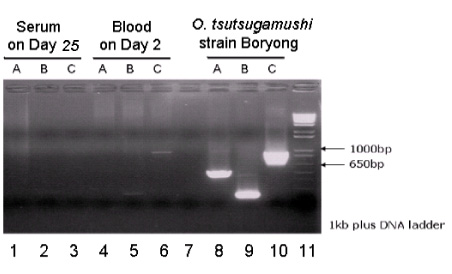
Figure 2 Gel electrophoresis of amplified DNAs by polymerase chain reaction of blood taken on admission shows bands of 272 bp and 1003 bp. No band is seen in the convalescent serum. A - primer TsuA (expected molecular size is 568 bp), B - primer SM1F (272 bp), and C - primer Gilliam (1003 bp). Lane 1-3, convalescent serum; Lane 4-6, blood on admission; Lane 7, blank; Lane 8-10, O. tsutsugamushi serotype Boryong as positive control; and Lane 11 contains molecular size markers.
Cited by 6 articles
-
In vitro Efficacy of Antibiotic Combinations against Orientia tsutsugamushi
Eun Sil Kim, Mee Kyung Kim, Hye Myung Lee, Moon-Hyun Chung, Jin-Soo Lee, Jae-Seung Kang
Infect Chemother. 2008;40(6):311-315. doi: 10.3947/ic.2008.40.6.311.Cholestatic Hepatitis Caused by Tongyeong Strain of Orientia tsutsugamushi
Kowoon Joo, Mee Kyung Kim, Se-Hee Kil, Moon-Hyun Chung, Joon-Mee Kim, Jae-Seung Kang
Infect Chemother. 2009;41(2):99-104. doi: 10.3947/ic.2009.41.2.99.First Case of Bartonella henselae Bacteremia in Korea
Jae-Hyoung Im, Ji Hyeon Baek, Hyun-Jung Lee, Jin-Soo Lee, Moon-Hyun Chung, Mijeong Kim, Sun Myoung Lee, Jae-Seung Kang
Infect Chemother. 2013;45(4):446-450. doi: 10.3947/ic.2013.45.4.446.History of Tsutsugamushi Disease in Korea
Moon-Hyun Chung, Jae-Seung Kang
Infect Chemother. 2019;51(2):196-209. doi: 10.3947/ic.2019.51.2.196.Treatment Guidelines for Community-acquired Pneumonia in Korea: An Evidence-based Approach to Appropriate Antimicrobial Therapy
Jae-Hoon Song, Ki-Suck Jung
J Korean Med Assoc. 2010;53(1):20-42. doi: 10.5124/jkma.2010.53.1.20.Treatment Guidelines for Community-acquired Pneumonia in Korea: An Evidence-based Approach to Appropriate Antimicrobial Therapy
Jae-Hoon Song, Ki-Suck Jung, Moon Won Kang, Do Jin Kim, Hyunjoo Pai, Gee Young Suh, Tae Sun Shim, Joong Hyun Ahn, Chul Min Ahn, Jun Hee Woo, Nam Yong Lee, Dong-Gun Lee, Mi Suk Lee, Sang Moo Lee, Yeong Seon Lee, Hyukmin Lee, Doo Ryeon Chung
Infect Chemother. 2009;41(3):133-153. doi: 10.3947/ic.2009.41.3.133.
Reference
-
1. Communicable diseases monthly report. Korea Centers for Diseases Control and Prevention;Available from: URL: http://stat.cdc.go.kr/DayWeekMonth/DiseasMonthOccur.aspx.2. Jang WH. Tsutsugamushi disease in Korea. 1994. Seoul: Seoheung Publishing Co..3. Kim MJ, Kim MK, Kang JS. Improved antibiotic susceptibility test of Orientia tsutsugamushi by flow cytometry using monoclonal antibody. J Korean Med Sci. 2007. 22:1–6.
Article4. Furuya Y, Yoshida Y, Katayama T, Yamamoto S, Kawamura A Jr. Serotype-specific amplification of Rickettsia tsutsugamushi DNA by nested polymerase chain reaction. J Clin Microbiol. 1993. 31:1637–1640.
Article5. Kim KA, Lee SH, Jang WS, Oh MD, Kim I, Choe K. Two cases of tsutsugamushi disease in the spring. Korean J Infect Dis. 1999. 31:46–49.6. Song HJ, Kim KH, Kim SC, Hong SS, Ree HI. Population density of chigger mites, the vector of tsutsugamushi disease in Chollanam-do, Korea. Korean J Parasitol. 1996. 34:27–33.
Article7. Kim MJ, Cheong HJ, Sohn JW, Shim HS, Park DW, Park SC, Woo JH, Kang JM, Kim YK, Shin WS, Kim YR, Lee HJ, Kim JH. A prospective multicenter study of the etiological analysis in adults with community-acquired pneumonia: legionella, leptospira, Hantaan virus and Orientia tsutsugamushi. Korean J Infect Dis. 2001. 33:24–31.8. Jang JG, Park PG, Lee HS, Maeng JH, Kim HS, Lee SC, Yoon SK, Choi JS. The study of 46 cases of tsutsugamushi disease in Young-Dong region in Gang-Won-Do. Infect Chemother. 2003. 35:138–144.9. Smadel JE. Influence of antibiotics on immunologic responses in scrub typhus. Am J Med. 1954. 17:246–258.
Article10. Kim JH, Jung KD, Kim SC, Lee SH, Jang WJ, Kim YW, Choi MS, Kim IS, Park KH. Serological analysis of epidemic typhus in Korea from 1990 to 1992. J Bacteriol Virol. 2001. 31:133–137.11. Graham JV, Baden L, Tsiodras S, Karchmer AW. Q fever endocarditis associated with extensive serological cross-reactivity. Clin Infect Dis. 2000. 30:609–610.
Article12. Heo ST, Park MY, Choi YS, Oh WS, Ko KS, Peck KR, Song JH. Q fever as a cause of fever of unknown origin. Korean J Med. 2008. 74:100–105.13. Park MS, Shim SK, Lee HK, Kim HR, Lee BC, Park MY. Laboratory diagnosis of Q fever by Coxiella burnetii infection (?). Rep Natl Inst Health. 2002. 38:65–78.14. Lever MS, Bewley KR, Dowsett B, Lloyd G. In vitro susceptibility of Coxiella burnetii to azithromycin, doxycycline, ciprofloxacin and a range of newer fluoroquinolones. Int J Antimicrob Agents. 2004. 24:194–196.15. Ralph A, Markey P, Schultz R. Q fever cases in the Northern Territory of Australia from 1991 to 2006. Commun Dis Intell. 2007. 31:222–227.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scrub typhus with complications of acute myocarditis and cardiac tamponade in metropolitan areas: two case reports
- Antibiotic Combination Therapy for Severe Scrub Typhus: Is It Necessary?
- A Case of Scrub Typhus with Bilateral Sudden Hearing Loss
- Severe Scrub Typhus Complicated by Myofascitis Due to the Taguchi Strain of Orientia tsutsugamushi
- Pulmonary Artery Thrombosis Associated with Scrub Typhus
