A Case of Pituitary Abscess that was Difficult to Diagnose due to Repeated Symptomatic Responses to Every Corticosteroid Administration
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. ldj6026@catholic.ac.kr
- 2Department of Neurosurgery, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2169128
- DOI: http://doi.org/10.3803/EnM.2011.26.1.72
Abstract
- Pituitary abscess is a rare pathology, but it is a potentially life-threatening condition. Therefore, timely intervention, including antibiotics and an operation, can prevent the morbidity and mortality in such cases. A 31-year-old woman, who was 16 months after her second delivery, presented with intermittent headache for 3 months. Amenorrhea, polyuria and polydipsia were noticed and the endocrinological hormone studies were compatible with panhypopituitarism and diabetes insipidus. Pituitary MRI demonstrated a 2.3 cm sized cystic mass with an upper small nodular lesion. Her symptoms such as headache and fever were repeatedly improved whenever corticosteroid was administered, which led us to suspect the diagnosis of an inflammatory condition like lymphocytic hypophysitis. During the hormone replacement therapy, her cystic pituitary mass had grown and her symptoms progressively worsened for another two months. The patient underwent trans-sphenoidal exploration and she turned out to have a pituitary abscess. At the 3-month follow-up, amenorrhea was noticed and her residual function of the pituitary was tested by a combined pituitary stimulation test. The results were compatible with panhypopituitarism. She received levothyroxine 100 microg, prednisolone 5 mg and desmopressin spray and she is being observed at the out-patient clinic. The authors experienced a patient with primary pituitary abscess that was confirmed pathologically and we report on its clinical course with a literature review.
MeSH Terms
-
Abscess
Adrenal Cortex Hormones
Adult
Amenorrhea
Anti-Bacterial Agents
Deamino Arginine Vasopressin
Diabetes Insipidus
Female
Fever
Follow-Up Studies
Headache
Hormone Replacement Therapy
Humans
Hypopituitarism
Outpatients
Polydipsia
Polyuria
Prednisolone
Thyroxine
Adrenal Cortex Hormones
Anti-Bacterial Agents
Deamino Arginine Vasopressin
Prednisolone
Thyroxine
Figure
-
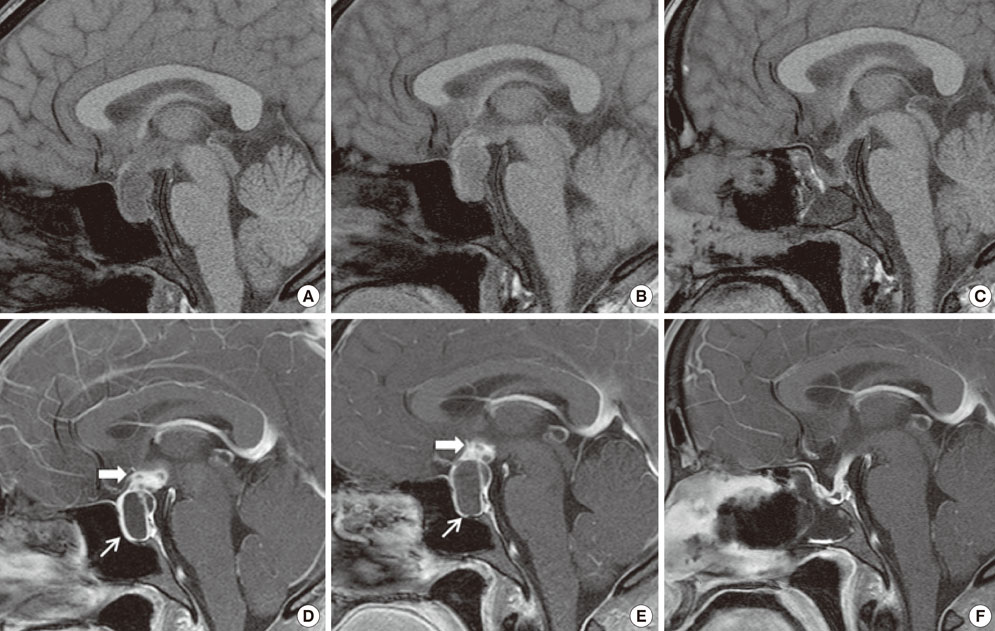
Fig. 1 Sella MRI; upper panels, T1-weighted images; lower panels, enhanced T1-weighted images. Initial sagittal images (A, D) show a 1.4 × 2.3 × 2.2 cm sized cystic mass (thin arrow) in sellar and suprasellar region with thickened stalk and a 1.4 cm sized enhancing nodular lesion (thick arrow) above the mass. 2 months later, preoperative sagittal images (B, E) show significant increase in size, extent and signal intensity of the cystic mass (thin arrow) and nodular contrast-enhancing lesion (thick arrow) on upper margin of the mass. Post-operative images (C, F) show that pituitary abscess was completely removed and normal pituitary gland was remaining with enhancement by gadolinium, along with pituitary stalk.
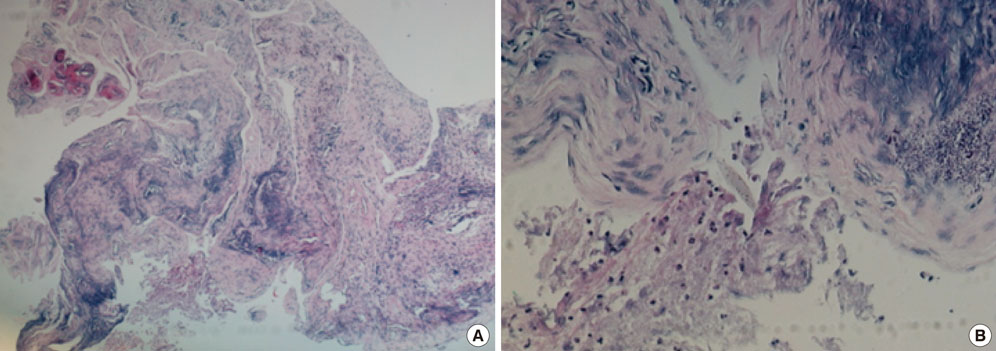
Fig. 2 Histology of the pituitary abscess. A, B. Polymorphonuclear neutrophil and fibrous tissue showing mild acute and chronic inflammation with focal necrosis and calcification (H&E staining, A, × 40, B, × 200).
Reference
-
1. Kim SS, Park KH, Jung SI, Jang MO, Kang SJ, Jung YS, Shin JH. A case of Klebsiella pneumoniae pituitary abscess cured by medical treatment. Korean J Med. 2009. 77:133–138.2. Lindholm J, Rasmussen P, Korsgaard O. Intrasellar or pituitary abscess. J Neurosurg. 1973. 38:616–619.3. Vates GE, Berger MS, Wilson CB. Diagnosis and management of pituitary abscess: a review of twenty-four cases. J Neurosurg. 2001. 95:233–241.4. Zhuchenko DG. Histogenesis and dynamics of formation of the wall of brain abscess in experimental conditions. Vopr Neirokhir. 1956. 20:20–30.5. Simmonds M. Zur pathologie der ag hypophysis. Verh Dtsch Pathol. 1914. 17:208–212.6. Domingue JN, Wilson CB. Pituitary abscesses. Report of seven cases and review of the literature. J Neurosurg. 1977. 46:601–608.7. Dutta P, Bhansali A, Singh P, Kotwal N, Pathak A, Kumar Y. Pituitary abscess: report of four cases and review of literature. Pituitary. 2006. 9:267–273.8. Dalan R, Leow MK. Pituitary abscess: our experience with a case and a review of the literature. Pituitary. 2008. 11:299–306.9. Asa SL, Bilbao JM, Kovacs K, Josse RG, Kreines K. Lymphocytic hypophysitis of pregnancy resulting in hypopituitarism: a distinct clinicopathologic entity. Ann Intern Med. 1981. 95:166–171.10. Hashimoto K, Takao T, Makino S. Lymphocytic adenohypophysitis and lymphocytic infundibuloneurohypophysitis. Endocr J. 1997. 44:1–10.11. Kim HC, Kang SG, Huh PW, Yoo do S, Cho KS, Kim DS. Pituitary abscess in a pregnant woman. J Clin Neurosci. 2007. 14:1135–1139.12. Kristof RA, Van Roost D, Klingmuller D, Springer W, Schramm J. Lymphocytic hypophysitis: non-invasive diagnosis and treatment by high dose methylprednisolone pulse therapy? J Neurol Neurosurg Psychiatry. 1999. 67:398–402.13. Dickob M, Scharphuis T, Distelmaier P, Hoffmann G. Diagnosis of hypophyseal abscess using MRI and high resolution CT. Neurochirurgia (Stuttg). 1989. 32:184–186.14. Bossard D, Himed A, Badet C, Lapras V, Mornex R, Fisher G, Tavernier T, Bochu M. MRI and CT in a case of pituitary abscess. J Neuroradiol. 1992. 19:139–144.15. Wolansky LJ, Gallagher JD, Heary RF, Malantic GP, Dasmahapatra A, Shaderowfsky PD, Budhwani N. MRI of pituitary abscess: two cases and review of the literature. Neuroradiology. 1997. 39:499–503.16. Blackett PR, Bailey JD, Hoffman HJ. A pituitary abscess simulating an intrasellar tumor. Surg Neurol. 1980. 14:129–131.17. Shirakawa J, Takeshita T, Miyao M, Orimo S, Terauchi Y, Mizuno Y. Pituitary abscess with panhypopituitarism showing T1 signal hyperintensity of the marginal pituitary area: a non-invasive differential diagnosis of pituitary abscess and pituitary apoplexy. Intern Med. 2009. 48:441–446.18. Carpinteri R, Patelli I, Casanueva FF, Giustina A. Pituitary tumours: inflammatory and granulomatous expansive lesions of the pituitary. Best Pract Res Clin Endocrinol Metab. 2009. 23:639–650.19. Beressi N, Beressi JP, Cohen R, Modigliani E. Lymphocytic hypophysitis. A review of 145 cases. Ann Med Interne (Paris). 1999. 150:327–341.
