Small Left Atrium: An Adjunctive Sign of Hemodynamically Compromised Massive Pulmonary Embolism
- Affiliations
-
- 1National Cancer Institute, NIH, Bethesda, MD, USA. yjhama2005@yahoo.co.jp
- 2Department of Radiology, National Defense Medical College, Tokorozawa, Japan.
- 3Internal Medicine, National Defense Medical College, Tokorozawa, Japan.
- KMID: 2158159
- DOI: http://doi.org/10.3349/ymj.2005.46.5.733
Abstract
- Pulmonary embolism (PE) is a common disease with a high mortality rate due to right ventricular dysfunction and underfilling of the left ventricle. We present a case of a 33-year-old man with hemodynamically compromised massive PE. His left atrium was collapsed with marked dilatation of the right atrium and ventricle on multi-detector-row CT scans. The patient was treated with an intracatheter injection of a mutant tissue-type plasminogen activator and subsequently showed clinical and radiological improvements. The small left atrial size in combination with a right ventricular pressure overload was considered to be an adjunctive sign of hemodynamically compromised massive PE.
Keyword
MeSH Terms
Figure
-

Fig. 1 Electrocardiogram at the time of admission showed an SI, QIII, TIII pattern.
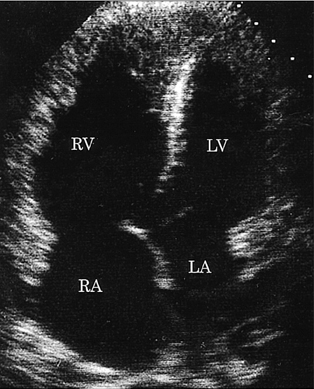
Fig. 2 Apical four-chamber view of the echocardiogram demonstrated marked dilatation of the right ventricle and right atrium. The interventricular septum and the atrial septum were deviated towards the left ventricle and left atrium respectively. RV, right ventricle; RA, right atrium; LV, left ventricle; LA, left atrium.
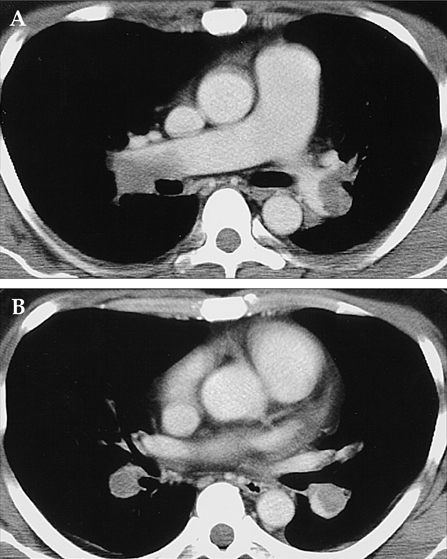
Fig. 3 A. Contrast-enhanced CT performed at the level of the right main pulmonary artery showed a large emboli in the bilateral main pulmonary arteries. B. Contrast-enhanced CT performed at the level of the descending interlobar pulmonary arteries showed low-attenuation emboli outlined by high attenuation contrast-enhanced flowing blood.
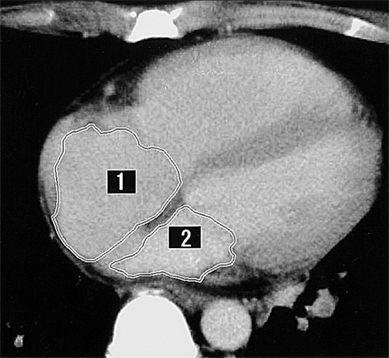
Fig. 4 Contrast-enhanced CT at the mid-ventricular level showed that the interventricular septum was straightened and the right ventricle and right atrium were dilated, indicating a raised pressure on the right side of the heart. The left atrium was markedly decreased in size, indicating underfilling of the left side of the heart. The region of interest was determined using contrast-enhanced CT scans. Each area (1 = right atrium; 2 = left atrium) was multiplied by its slice thickness (8 mm) and the results were added together using the workstation (Fiji Photo Film Co., Ltd., Tokyo, Japan).
Reference
-
1. Dalen JE, Alpert JS. Natural history of pulmonary embolism. Prog Cardiovasc Dis. 1975. 17:257–270.2. Barritt DW, Jordan SC. Anticoagulant drugs in the treatment of pulmonary embolism. A controlled trial. Lancet. 1960. 1:1309–1312.3. De Monye W, Pattynama PMT. Contrast-enhanced spiral computed tomography of the pulmonary arteries; an overview. Semin Thromb Hemost. 2001. 7:33–39.4. Van Strijen MJ, de Monye W, Kieft GJ, Pattynama PM, Huisman MV, Smith SJ, et al. Diagnosis of pulmonary embolism with spiral CT as a second procedure following scintigraphy. Eur Radiol. 2003. 13:1501–1507.5. Blachere H, Latrabe V, Montaudon M, Valli N, Couffinhal T, Raherisson C, et al. Pulmonary embolism revealed on helical CT angiography: comparison with ventilation-perfusion radionuclide lung scanning. Am J Roentgenol. 2000. 174:1041–1047.6. Hirasawa K, Okamoto M. Cardiovascular anatomy. Buntankaibougaku. 1982. Tokyo, Japan: Kanehara & Co., Ltd.;6–17. (in Japanese).7. Contractor S, Maldjian PD, Sharma VK, Gor DM. Role of helical CT in detecting right ventricular dysfunction secondary to acute pulmonary embolism. J Comput Assist Tomogr. 2002. 26:587–591.8. Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002. 21:877–905.9. Hiorns MP, Mayo JR. Spiral computed tomography for acute pulmonary embolism. Can Assoc Radiol J. 2002. 53:258–268.10. Mastora I, Remy-Jardin M, Masson P, Galland E, Delannoy V, Bauchart JJ, et al. Severity of acute pulmonary embolism: evaluation of a new spiral CT angiographic score in correlation with echocardiographic data. Eur Radiol. 2003. 13:29–35.11. Rosenquist GC, Kelly JL, Chandra R, Ruckman RN, Galioto FM Jr, Midgley FM, et al. Small left atrium and change in contour of the ventricular septum in total anomalous pulmonary venous connection: a morphometric analysis of 22 infant hearts. Am J Cardiol. 1985. 55:777–782.12. Hofmann LK, Becker CR, Flohr T, Schoepf UJ. Multidetector-row CT of the heart. Semin Roentgenol. 2003. 38:135–145.13. Hama Y, Kusano S. Picture archiving and communication system: prospective study. Hong Kong Med J. 2002. 8:21–25.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A fluttering worm-like thrombus-in-transit in the right atrium: A sign of disastrous embolism
- A Massive Pulmonary Embolism with Hemodynamically Unstable Stroke Symptoms
- A Case of Impending Paradoxical Embolus in a Patient with Acute Pulmonary Embolism
- Massive Pulmonary Embolism with Thrombus-in-Transit Entrapped by a Patent Foramen Ovale
- Anesthetic Management of Pulmonary Embolectomy
