Endoscopic Dacryocystorhinostomy: Creation of a Large Marsupialized Lacrimal Sac
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University Boramae Hospital, Seoul, Korea. hrjin@paran.com
- 2Department of Otolaryngology, Chungbuk National University Hospital, Cheongju, Korea.
- 3Department of Ophthalmology, Chungbuk National University Hospital, Cheongju, Korea.
- KMID: 2157827
- DOI: http://doi.org/10.3346/jkms.2006.21.4.719
Abstract
- This retrospective study describes and evaluates the effectiveness of a modified technique of conventional endoscopic dacryocystorhinostomy (DCR) that minimizes the obstruction of a neo-ostium by creating an enlarged marsupialized lacrimal sac using mucosal flaps. Forty-two patients who had undergone 46 endoscopic DCR at a tertiary medical center, from 2002 to 2004, for correction of lacrimal system obstruction were investigated. The surgical technique involves elevation of a nasal mucosal flap, full sac exposure using a power drill, and shaping of the mucosal flap to cover denuded bone and juxtapose exposed sac mucosa. Postoperative symptoms and endoscopic findings of the neo-ostium were evaluated. Mean duration of follow-up was 5.9 months. An eighty-three percent primary success rate was observed, without any serious complications. Obstruction of the neo-ostium with granulation tissue was observed in eight cases, among which six underwent revision with success in all cases. Overall, 44 (96%) of 46 cases experienced surgical successes. Endoscopic DCR, a procedure in which a large marsupialized lacrimal sac is created from mucosal flaps, yields a very satisfactory success rate with straightforward and highly successful revision available for those in whom the primary procedure yields a substandard result.
MeSH Terms
Figure
-
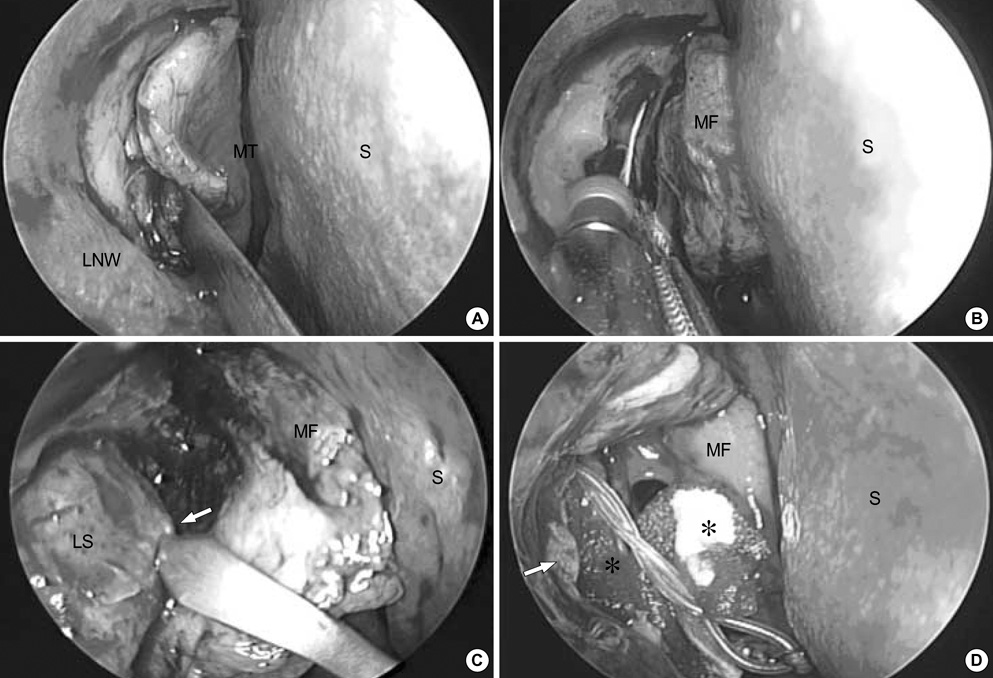
Fig. 1 (A) A nasal mucosal flap is being elevated after a reverse "C" shaped incision on the mucosa of the lateral nasal wall with slit knife just anterior to the insertion of middle turbinate. (B) The maxillary bone covering the lacrimal sac is drilled out with a curved diamond dacryocystorhinostomy bur (15°, 2.9 mm, Xomed Co., Jacksonville, Florida, U.S.A.). (C) The extent of the lacrimal sac is verified with lacrimal probe (arrow) and the sac wall is tented to allow incision. The vertical incision is made with a slit knife. (D) The mucosal flap covers the exposed bony portion after cutting and trimming. The edges of the exposed lacrimal sac (arrow) are everted to match the nasal mucosa and the sac lumen is filled with gelfoam (asterisk) to keep the flap anastomosis in position. A silicone bicannalicular tube is seen through the new opening. LNW, lateral nasal wall; MT, middle turbinate; S, septum; LS, lacrimal sac; MF, mucosal flap.

Fig. 2 A wide neo-ostium made by marsupialization of the lacrimal sac (arrow) at six months after surgery. MT indicates the middle turbinate.
Cited by 1 articles
-
Results of Endonasal Dacryocystorhinostomy with Lacrimal Sac Flap and Silastic Sheet
Hyun Duk Jang, Sang Soo Kim
J Korean Ophthalmol Soc. 2011;52(12):1391-1398. doi: 10.3341/jkos.2011.52.12.1391.
Reference
-
1. Jones LT. The cure of epiphora due to canalicular disorders, trauma and surgical failures on the lacrimal passages. Trans Am Acad Ophthalmol Otolaryngol. 1962. 66:506.2. McDonough M, Meiring JH. Endoscopic transnasal dacryocystorhinostomy. J Laryngol Otol. 1989. 103:585–587.3. Watkins LM, Janfaza P, Rubin PA. The evolution of endonasal dacryocystorhinostomy. Surv Ophthalmol. 2003. 48:73–84.
Article4. Hartikainen J, Antila J, Varpula M, Puukka P, Seppa H, Grenman R. Prospective randomized comparison of endonasal endoscopic dacryocystorhinostomy and external dacryocystorhinostomy. Laryngoscope. 1998. 108:1861–1866.
Article5. Ben Simon GJ, Joseph J, Lee S, Schwarcz RM, McCann JD, Goldberg RA. External versus endoscopic dacryocystorhinostomy for acquired nasolacrimal duct obstruction in a tertiary referral center. Ophthalmology. 2005. 112:1463–1468.
Article6. Ibrahim HA, Batterbury M, Banhegyi G, McGalliard J. Endonasal laser dacryocystorhinostomy and external dacryocystorhinostomy outcome profile in a general ophthalmic service unit: a comparative retrospective study. Ophthalmic Surg Lasers. 2001. 32:220–227.
Article7. Tsirbas A, Davis G, Wormald PJ. Revision dacryocystorhinostomy: a comparison of endoscopic and external techniques. Am J Rhinol. 2005. 19:322–325.
Article8. Massaro BM, Gonnering RS, Harris GJ. Endonasal laser dacryocystorhinostomy: A new approach to nasolacrimal duct obstruction. Arch Ophthalmol. 1990. 108:1172–1176.9. Metson R, Woog JJ, Puliafito CA. Endoscopic laser dacryocystorhinostomy. Laryngoscope. 1994. 104:269–274.
Article10. Zilelioglu G, Tekeli O, Ugurba SH, Akiner M, Akturk T, Anadolu Y. Results of endoscopic endonasal non-laser dacryocystorhinostomy. Doc Ophthalmol. 2002. 105:57–62.11. Gurler B, San I. Long-term follow-up outcomes of nonlaser intranasal endoscopic dacryocystorhinostomy: how suitable and useful are conventional surgical instruments? Eur J Ophthalmol. 2004. 14:453–460.
Article12. Sham CL, van Hasselt CA. Endoscopic terminal dacryocystorhinostomy. Laryngoscope. 2000. 110:1045–1049.
Article13. Selig YK, Biesman BS, Rebeiz EE. Topical application of mitomycin-C in endoscopic dacryocystorhinostomy. Am J Rhinol. 2000. 14:205–207.
Article14. Park DJ, Kwak MS. The effect of mitomycin-C on the success rate of endoscopic dacryocystorhinostomy. J Korean Ophthalmol Soc. 2000. 41:1674–1679.15. Wormald PJ. Powered endoscopic dacryocystorhinostomy. Laryngoscope. 2002. 112:69–72.
Article16. Tsirbas A, Wormald PJ. Mechanical endonasal dacryocystorhinostomy with mucosal flaps. Br J Ophthalmol. 2003. 87:43–47.
Article17. Massegur H, Trias E, Adema JM. Endoscopic dacryocystorhinostomy: modified technique. Otolaryngol Head Neck Surg. 2004. 130:39–46.
Article18. Ozturk S, Konuk O, Ilgit ET, Unal M, Erdem O. Outcome of patients with nasolacrimal polyurethane stent implantation: do they keep tearing? Ophthal Plast Reconstr Surg. 2004. 20:130–135.19. Unlu HH, Toprak B, Aslan A, Guler C. Comparison of surgical outcomes in primary endoscopic dacryocystorhinostomy with and without silicone intubation. Ann Otol Rhinol Laryngol. 2002. 111:704–709.
Article20. Mortimore S, Banhegy GY, Lancaster JL, Karkanevatos A. Endoscopic dacryocystorhinostomy without silicone stenting. J R Coll Surg Edinb. 1999. 44:371–373.21. Lee TS, Kim SW. The effects of placement of bicanalicular silicone tube and silicone stent on granuloma formation in endoscopic intranasal dacryocystorhinostomy. J Korean Ophthalmol Soc. 1999. 40:16–22.22. Fayet B, Racy E, Assouline M. Complications of standardized endonasal dacryocystorhinostomy with unciformectomy. Ophthalmology. 2004. 111:837–845.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Success Rate of Endonasal Dacryocystorhinostomy Based on the Location of the Lacrimal Sac
- Endoscopic Dacryocystorhinostomy for the Treatment of Lacrimal Sac Abscess
- The Role of Dacryocystography in Evaluation of Nasolacrimal Duct Obstruction
- The Correlation between Organisms Cultured from the Lacrimal Sac and Lacrimal Punctum in Dacryocystitis
- Posterior Lacrimal Sac Approach in Endoscopic Dacryocystorhinostomy
