A Case of Myocardial Abscess Mimicking Acute Myocardial Infarction
- Affiliations
-
- 1Department of Cardiology, The Heart Center, Chonnam National University Hospital, Gwangju, Korea. jcpark54@hanmail.net
- KMID: 2135448
- DOI: http://doi.org/10.4250/jcu.2009.17.2.73
Abstract
- Myocardial abscess, a rare and life-threatening disease, occurs as a complication of infective endocarditis, acute myocardial infarction, or other infections in the setting of debilitating condition. We report a case of myocardial abscess mimicking acute myocardial infarction (AMI), not a following consequence of AMI. We can diagnose the disease with the aid of transthoracic echocardiography and cardiac computed tomography.
Keyword
Figure
-

Fig. 1 Electrocardiogram on admission (A) shows ST segment elevations and T wave inversions in the anterior leads. Follow-up electrocardiogram checked 7 weeks later after the first exam (B) reveals normalization of ST-segment abnormality.
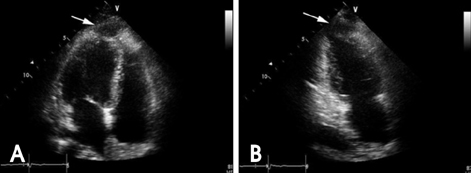
Fig. 2 Apical 4 chamber view (A) and apical 2 chamber view (B) of transthoracic echocardiography on admission shows hypoechoic lesion (arrow) at the myocardium just adjacent hypokinetic apical area. Note that the maximal size was 27.2×11.9 mm.
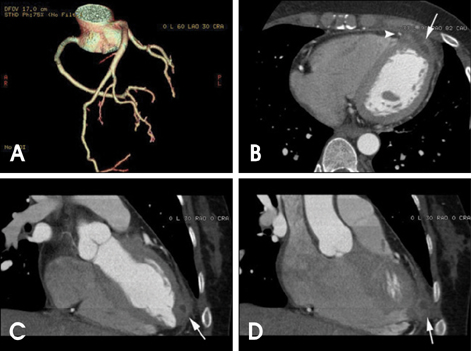
Fig. 3 Volume rendering image (A) of cardiac computed tomography shows no critical narrowing in either coronary arteries. Cardiac computed tomography (B, C and D) demonstrates mild diffuse thickening with contrast enhancement of apical myopericardium and loculated fluid collection in the area (arrows). Note that left anterior descending coronary artery runs beside the lesion (arrowhead in panel B).

Fig. 4 2D Echocardiogram performed 2 weeks later (A and B) shows no significant interval change of lesion size. 2D echocardiogram carried out 7 weeks later (C and D) demonstrates complete resolution of the lesion.

Fig. 5 Follow-up chest computed tomography after 3 weeks of antibiotics treatment shows markedly decreased lesion, but still remained focal wall thickening and enhancement.
Reference
-
1. Iqbal J, Ahmed I, Baiq W. Metastatic myocardial abscess on the posterior wall of the left ventricle: a case report. J Med Case Reports. 2008. 2:258.
Article2. Chikwe J, Barnard J, Pepper JR. Myocardial abscess. Heart. 2004. 90:597.
Article3. Behnam R, Walter S, Hanes V. Myocardial abscess complicating myocardial infarction. J Am Soc Echocardiogr. 1995. 8:334–337.
Article4. Ghani M, Boughner D. Echocardiographic diagnosis of myocardial abscess complicating myocardial infarction. J Am Soc Echocardiogr. 1994. 7:318–320.
Article5. Choi SI, Shin DH, Shin JH, Lee JU, Kim SK, Kim KS, Lim HK, Kim JH, Lee BH. A case of aortic root abscess causing fatal myocardial infarction. J Cardiovasc Ultrasound. 2006. 14:63–66.
Article6. Khan B, Strate RW, Hellman R. Myocardial abscess and fatal cardiac arrhythmia in a hemodialysis patient with an arterio-venous fistula infection. Semin Dial. 2007. 20:452–454.
Article7. Vega Moller D, Bruun NE. Substantial myocardial abscess in an immunocompromised patient: Fatal outcome after coagulase-negative Staphylococcal native valve infection. J Am Soc Echocardiogr. 2007. 20:333.e5–333.e8.
Article8. Chakrabarti J. Diagnostic evaluation of myocardial abscess. A new look at an old problem. Int J Cardiol. 1995. 52:189–196.
Article9. Hill EE, Herijgers P, Claus P, Vanderschueren S, Peetermans WE, Herregods MC. Abscess in infective endocarditis: The value of transesophageal echocardiography and outcome: A 5-year study. Am Heart J. 2007. 154:923–928.
Article10. Shackcloth MJ, Dihmis WC. Contained rupture of a myocardial abscess in the free wall of the left ventricle. Ann Thorac Surg. 2001. 72:617–619.
Article11. Khan B, Strate RW, Hellman R. Myocardial abscess and fatal cardiac arrhythmia in a hemodialysis patient with an arterio-venous fistula infection. Semin Dial. 2007. 20:452–454.
Article12. Fredenrich A, Jourdan J, Gibelin P, Vinti H, Taillan B, Bossan S, Baudouy M, Morand P. Ventricular arrhythmias disclosing myocardial abscess in infectious mitro-aortic endocarditis. Ann Cardiol Angeiol (Paris). 1990. 39:531–533.13. Javaid M, Awasthi A, Fink G. Complete heart block associated with mitral annular abscess. Mayo Clin Proc. 2005. 80:1531–1532.
Article14. Lammers J, van Dantzig JM. PR prolongation in aortic root abscess. Heart. 2005. 91:1474.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Treatment of Acute Myocardial Infarction: What is the Optimal Therapy for Acute Myocardial Infarction?
- A Case of Acute Myopericarditis with Localized ST Elevation Mimicking Myocardial Infarction
- Myocardial fractional flow reserve in acute myocardial infarction
- Coronary Slow Flow Phenomenon Leads to ST Elevation Myocardial Infarction
- A Case of Non-Q Myocardial Infaction in a Patient with Myocardial Bridging
