J Korean Foot Ankle Soc.
2015 Dec;19(4):193-196. 10.14193/jkfas.2015.19.4.193.
Melorheostosis with Synovial Chondromatosis of the Foot: A Report of Two Cases
- Affiliations
-
- 1Department of Orthopedic Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. fbbksw@hanmail.net
- 2Department of Pathology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 2132464
- DOI: http://doi.org/10.14193/jkfas.2015.19.4.193
Abstract
- Melorheostosis is a rare disease, belonging to the sclerotic bone dysplasia group. Initially described by Leri and Joanny in 1922, its etiology remains unknown. Onset is usually insidious, with deformity of the extremity, pain, limb stiffness, and limitation of motion in the joints. The typical radiographic appearance consists of irregular hyperostotic changes of the cortex, resembling melted wax dripping down one side of a candle. Treatment is usually symptomatic and conservative; however, conservative treatment is unsatisfactory due to functional issues when involving the distal extremity. We report on two cases of melorheostosis with synovial chondromatosis of the foot treated by mass excision.
Keyword
MeSH Terms
Figure
-

Figure 1. Preoperative anteroposterior plain radiography shows several sclerotic changes in the fourth metatarsal bone and irregular flowing hyperostosis along fourth metatarsal bone.
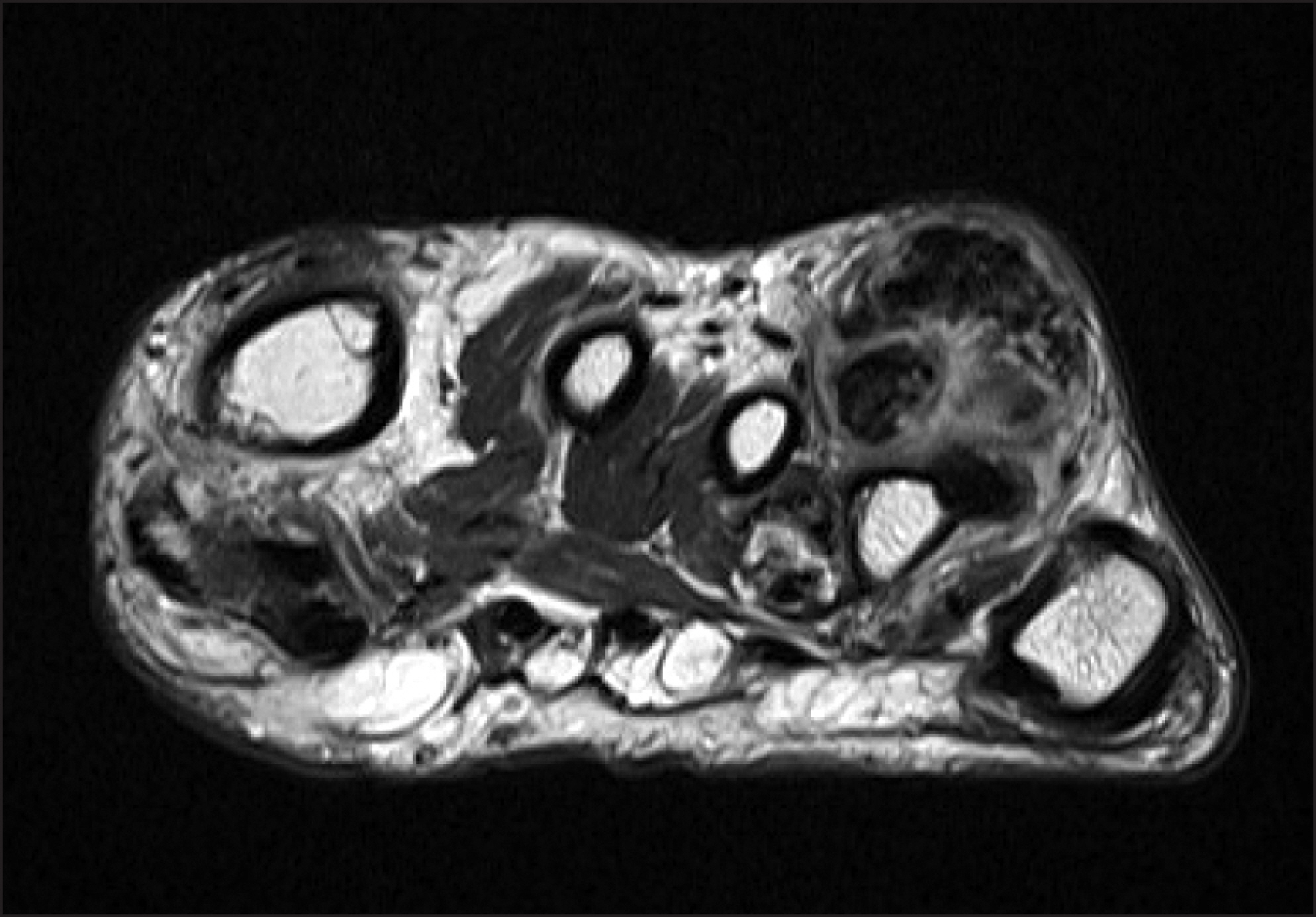
Figure 2. An axial T2-weighted magnetic resonance image of melorheostosis patient shows low signal intensity juxtacortical nodular lesion in the dorsal aspect of the fourth metatarsal bone.

Figure 3. The dorsal surface of the bony mass was exposed during operation.

Figure 4. Postoperative anteroposterior plain radiography shows complete excision of irregular flowing hyperostosis.
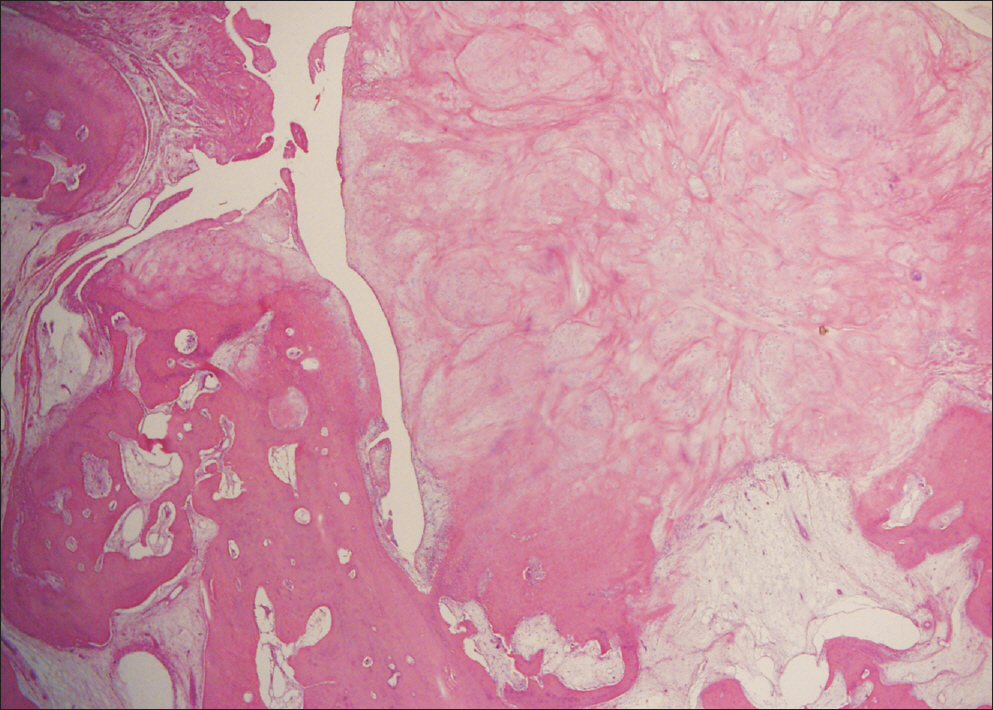
Figure 5. A photomicrograph shows melorheostosis and synovial chondromatosis (H&E stain, ×40).
Reference
-
References
1. Jain VK, Arya RK, Bharadwaj M, Kumar S. Melorheostosis: clinicopathological features, diagnosis, and management. Orthopedics. 2009; 32:512–20.
Article2. Suresh S, Muthukumar T, Saifuddin A. Classical and unusual imaging appearances of melorheostosis. Clin Radiol. 2010; 65:593–600.
Article3. Lester CW. Melorheostosis in a prehistoric Alaskan skeleton. J Bone Joint Surg Am. 1967; 49:142–3.
Article4. Greenspan A, Azouz EM. Bone dysplasia series. Melorheostosis: review and update. Can Assoc Radiol J. 1999; 50:324–30.5. Moore JJ, de Lorimier AA. Melorheostosis Leri: review of literature and report of a case. Am J Roentgenol Radium Ther. 1933; 29:161–71.6. Murray RO, McCredie J. Melorheostosis and the sclerotomes: a radiological correlation. Skeletal Radiol. 1979; 4:57–71.
Article7. Fryns JP. Melorheostosis and somatic mosaicism. Am J Med Genet. 1995; 58:199.
Article8. Campbell CJ, Papademetriou T, Bonfiglio M. Melorheostosis: a report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am. 1968; 50:1281–304.9. Judkiewicz AM, Murphey MD, Resnik CS, Newberg AH, Temple HT, Smith WS. Advanced imaging of melorheostosis with emphasis on MRI. Skeletal Radiol. 2001; 30:447–53.
Article10. Yu JS, Resnick D, Vaughan LM, Haghighi P, Hughes T. Melorheostosis with an ossified soft tissue mass: MR features. Skeletal Radiol. 1995; 24:367–70.
Article
