Microsurgical Strategies Following Failed Endovascular Treatment with the Pipeline Embolization Device: Case of a Giant Posterior Cerebral Artery Aneurysm
- Affiliations
-
- 1Department of Neurological Surgery, University of Virginia, Charlottesville, VA, United States. kcl3j@hscmail.mcc.virginia.edu
- KMID: 2055281
- DOI: http://doi.org/10.7461/jcen.2014.16.1.26
Abstract
- Treatment of giant posterior circulation aneurysms, via endovascular or microsurgical approaches, carries a high risk of morbidity and mortality. While flow-diverting stents (FDSs) represent a potent therapy for endovascular reconstruction of complex aneurysms, they are also associated with novel complications for which effective salvage techniques are lacking. We present a unique complication from failed treatment with a FDS. A 51 year-old male presented with increasing headaches secondary to a giant, fusiform aneurysm of the left posterior cerebral artery, which was largely thrombosed. Due to progressive enlargement of the aneurysm corresponding to worsening clinical symptoms, the lesion was treated with two Pipeline embolization devices (ev3, Plymouth, MN, United States). Three months after Pipeline embolization device treatment, complete posterior cerebral artery occlusion was observed at the origin of the proximal stent. Despite the lack of arterial inflow, the aneurysm dome continued to grow, resulting in obstructive hydrocephalus. Therefore microsurgical intervention was undertaken to trap and excise the aneurysm. The patient's postoperative course was complicated by multiple venous infarcts, ultimately resulting in death. Successful microsurgical obliteration of aneurysms previously treated with FDSs is extremely difficult. A combination of judicious preoperative planning and meticulous intraoperative surgical technique are requisite for effective management of these complicated cases.
Keyword
MeSH Terms
Figure
-
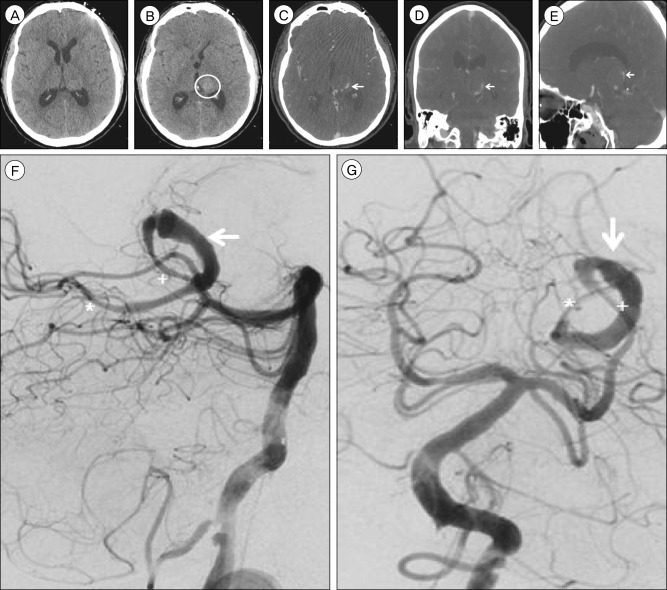
Fig. 1 Non-contrast brain computed tomography (CT), axial view, (A) shows no evidence of obstructive hydrocephalus and (B) demonstrates a round, hyperdense structure (circle) in the region of the left thalamus compatible with the partially thrombosed aneurysm sac arising from the left posterior cerebral artery (PCA) previously diagnosed. The intra-aneurysmal thrombotic mass measures 21×21 mm, increased from 17×18 mm 10 weeks prior and from 14×14 mm eight months prior. Brain CT angiography (CTA), (C) axial, (D) coronal, and (E) sagittal views, demonstrates an irregular, fusiform dilatation of the left PCA P2 and P3 segments (arrow) with a largely thrombosed aneurysm sac arising medially. Cerebral angiography, lateral (F) and anteroposterior (G) views, demonstrates a giant, fusiform aneurysm of the left distal PCA P2 and P3 segments with a similar serpentine morphology (arrow) compared to prior angiography 10 months prior. The aneurysm measures approximately 40 mm in length and its proximal dilatation has increased in size to 4.5 mm from 3.7 mm on previous angiography. Arterial flow through the diseased segment of the parent artery is mildly delayed, and the majority of the aneurysm sac known to be thrombosed from non-invasive imaging (B-E). The diameter of the parent PCA vessel is 1.3 mm. The aneurysm was treated with two telescoping pipeline embolization devices, 2.5×20 mm and 3.0×35 mm in size, without complications. The proximal (+) and distal (*) ends of the dual PED construct are marked (F, G).
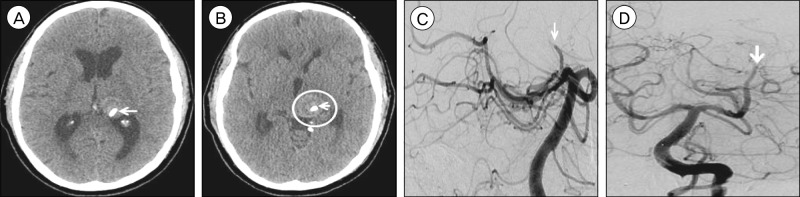
Fig. 2 Non-contrast brain computed tomography (CT), axial view, performed six weeks after pipeline embolization device (PED) treatment demonstrates (A) interval development of obstructive hydrocephalus due to (B) enlargement of the hyperdense intra-aneurysmal thrombus (circle) to 24×24 mm from 21×21 mm previously, resulting in increased mass effect upon the posterior aspect of the third ventricle. The previously deployed PEDs (arrow) are visualized within the diseased parent artery (A, B). Cerebral angiography, lateral (C) and anteroposterior (D) views, performed three months after PED treatment demonstrates thrombosis of the left PCA at the P2 segment (arrow). The origin of the thrombosis corresponds to the origin of the proximal PED.
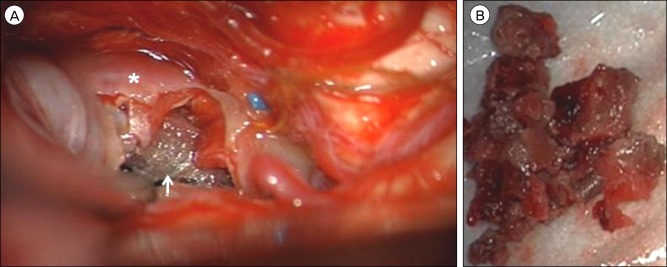
Fig. 3 Following an infratemporal, post-auricular, presigmoid skull base approach to the middle fossa, the (A) aneurysm dome (asterisk) was visualized superior to the tentorial incisura through a subtemporal corridor. After the aneurysm dome was excised, the pipeline embolization device (arrow) was identified within the lumen of the diseased parent posterior cerebral artery. (B) Gross examination of the debulked thrombus removed from the aneurysm sac.
Cited by 2 articles
-
Endovascular Management of Intracranial Aneurysms: Advances in Stenting Techniques and Technology
Dale Ding
J Cerebrovasc Endovasc Neurosurg. 2015;17(4):331-333. doi: 10.7461/jcen.2015.17.4.331.Delayed Ischemic Stroke after Flow Diversion of Large Posterior Communicating Artery Aneurysm
Si On Kim, Yeon Gu Chung, Yu Sam Won, Myung Ho Rho
J Cerebrovasc Endovasc Neurosurg. 2016;18(1):19-26. doi: 10.7461/jcen.2016.18.1.19.
Reference
-
1. International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms - Risk of rupture and risks of surgical intervention. N Engl J Med. 1998; 12. 339(24):1725–1733. PMID: 9867550.2. Arrese I, Sarabia R, Pintado R, Delgado-Rodriguez M. Flow-diverter devices for intracranial aneurysms: Systematic review and meta-analysis. Neurosurgery. 2013; 8. 73(2):193–200. discussion 199-200. PMID: 23624409.3. Cantore G, Santoro A, Guidetti G, Delfinis CP, Colonnese C, Passacantilli E. Surgical treatment of giant intracranial aneurysms: Current viewpoint. Neurosurgery. 2008; 10. 63(4 Suppl 2):279–289. discussion 289-90. PMID: 18981833.
Article4. Dehdashti AR, Thines L, Willinsky RA, Tymianski M. Symptomatic enlargement of an occluded giant carotido-ophthalmic aneurysm after endovascular treatment: The vasa vasorum theory. Acta Neurochir (Wien). 2009; 9. 151(9):1153–1158. PMID: 19343269.
Article5. Ding D, Liu KC. Microsurgical extraction of a malfunctioned pipeline embolization device following complete deployment. J Cerebrovasc Endovasc Neurosurg. 2013; 9. 15(3):241–245. PMID: 24167807.
Article6. Drake CG. Giant intracranial aneurysms: Experience with surgical treatment in 174 patients. Clin Neurosurg. 1979; 26:12–95. PMID: 544122.
Article7. Kim YB, Lee JW, Huh SK, Kim BM, Kim DJ. Outcomes of multidisciplinary treatment for posterior cerebral artery aneurysms. Clin Neurol Neurosurg. 2013; 10. 115(10):2062–2068. PMID: 23910998.
Article8. Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, Hashimoto N, et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 2012; 6. 366(26):2474–2482. PMID: 22738097.
Article9. Nelson PK, Lylyk P, Szikora I, Wetzel SG, Wanke I, Fiorella D. The pipeline embolization device for the intracranial treatment of aneurysms trial. AJNR Am J Neuroradiol. 2011; 1. 32(1):34–40. PMID: 21148256.
Article10. Parkinson RJ, Eddleman CS, Batjer HH, Bendok BR. Giant intracranial aneurysms: Endovascular challenges. Neurosurgery. 2006; 11. 59(5 Suppl 3):S103–S112. discussion S3-13. PMID: 17053593.
Article11. Pistocchi S, Blanc R, Bartolini B, Piotin M. Flow diverters at and beyond the level of the circle of willis for the treatment of intracranial aneurysms. Stroke. 2012; 4. 43(4):1032–1038. PMID: 22282890.
Article12. Wajnberg E, Silva TS, Johnson AK, Lopes DK. Progressive deconstruction: A novel aneurysm treatment using the pipeline embolization device for competitive flow diversion. Neurosurgery. 2014; 3. 10(Suppl 1):E161–E166. PMID: 23787883.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microsurgical Strategies Following Failed Endovascular Treatment with the Pipeline Embolization Device: Case of a Giant Posterior Cerebral Artery Aneurysm
- Microsurgical Extraction of a Malfunctioned Pipeline Embolization Device Following Complete Deployment
- Inadvertent Complication of a Pipeline Embolization Device for Treatment with Vertebral Artery Dissecting Aneurysm : Distal Tip Fracture of Delivery Wire
- Balloon Anchor Technique for Pipeline Embolization Device Deployment Across the Neck of a Giant Intracranial Aneurysm
- Dissecting Aneurysm of the Posterior Cerebral Artery Masquerading as Saccular Giant Aneurysm
