Endovascular Recanalization of a Thrombosed Native Arteriovenous Fistula Complicated with an Aneurysm: Technical Aspects and Outcomes
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, College of Medicine, Seoul National University, Seoul 110-744, Korea.
- 2Department of Radiology, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul 156-707, Korea. sorock71@snu.ac.kr
- 3Department of Surgery, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul 156-707, Korea.
- KMID: 2070179
- DOI: http://doi.org/10.3348/kjr.2015.16.2.349
Abstract
OBJECTIVE
To evaluate the technical aspects and outcomes of endovascular recanalization of a thrombosed native arteriovenous fistula (AVF) complicated with an aneurysm.
MATERIALS AND METHODS
Sixteen patients who had a thrombosed AVF complicated with an aneurysm (two radiocephalic and 14 brachiocephalic) were included in this study. Recanalization procedures were performed by mechanical thrombectomy using the Arrow-Trerotola percutaneous thrombectomy device and adjunctive treatments. We evaluated dose of thrombolytic agent, underlying stenosis, procedure time, technical and clinical success, and complications. The primary and secondary patency rates were calculated using the Kaplan-Meier analysis.
RESULTS
The thrombolytic agents used were 100000 U urokinase mixed with 500 IU heparin (n = 10) or a double dose of the mixture (n = 6). The thrombi in aneurysms were removed in all but two patients with non-flow limiting residual thrombi. One recanalization failure occurred due to a device failure. Aspiration thrombectomy was performed in 87.5% of cases (n = 14). Underlying stenoses were found in the outflow draining vein (n = 16), arteriovenous anastomosis or juxtaanastomosis area (n = 5), and the central vein (n = 3). Balloon angioplasty was performed for all stenoses in 15 patients. Two patients with a symptomatic central vein stenosis underwent insertion of a stent after balloon angioplasty. Mean procedure time was 116.3 minutes. Minor extravasation (n = 1) was resolved by manual compression. Both technical and clinical success rates were 93.8% (n = 15). The primary patency rates at 3, 6, and 12 months were 70.5%, 54.8%, and 31.3%, respectively. The secondary patency rates at 3, 6, and 12 months were 70.5%, 70.5%, and 47.0%, respectively.
CONCLUSION
Thrombosed AVF complicated with an aneurysm can be successfully recanalized, and secondary patency can be prolonged with endovascular treatment.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Aneurysm/complications/*surgery
Angioplasty, Balloon
Arteriovenous Fistula/*surgery
Arteriovenous Shunt, Surgical/adverse effects
Constriction, Pathologic/complications
Endovascular Procedures
Equipment Failure
Female
Fibrinolytic Agents/therapeutic use
Heparin/therapeutic use
Humans
Kaplan-Meier Estimate
Male
Middle Aged
Retrospective Studies
Stents/adverse effects
Thrombectomy/instrumentation/*methods
Thrombosis/etiology/*surgery
Urokinase-Type Plasminogen Activator/therapeutic use
Vascular Patency
Veins
Fibrinolytic Agents
Heparin
Urokinase-Type Plasminogen Activator
Figure
-
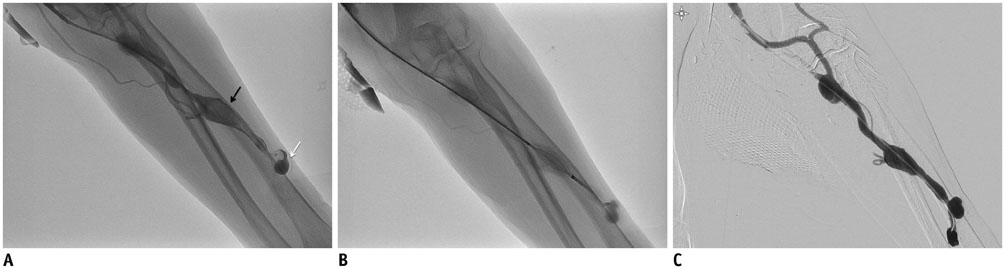
Fig. 1 86-year-old woman with radiocephalic arteriovenous fistula (AVF) in left forearm vein. A. Fistulogram obtained through retrograde puncture of draining vein shows > 50% thrombosis in draining vein. Saccular (white arrow) and diffuse aneurysms (black arrow) are shown on fistulogram. B. Mechanical thrombectomy was performed with percutaneous thrombectomy device to fragment thrombi. C. After aspiration thrombectomy and balloon angioplasty for stenotic segment. Catheter was advanced into arteriovenous anastomosis site to complete fistulogram. Fistulogram showing that flow through radiocephalic AVF was restored without limitation and without residual thrombi.
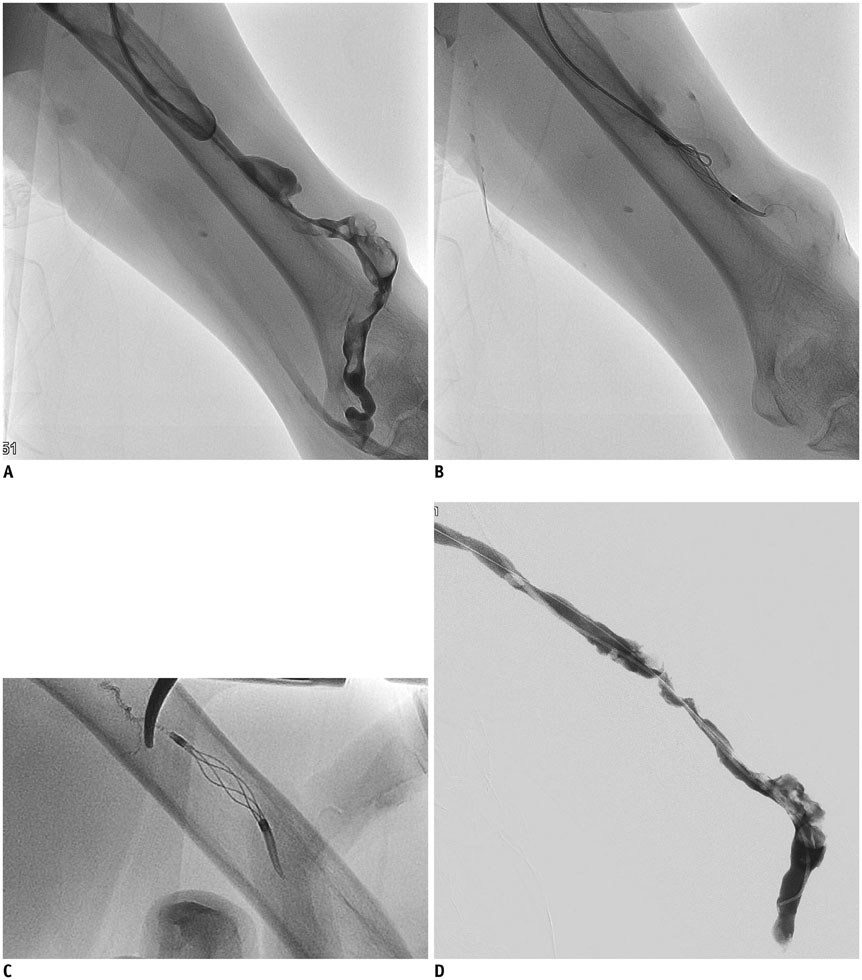
Fig. 2 57-year-old man with brachiocephalic arteriovenous fistula in left upper arm. A. Fistulogram obtained through retrograde puncture of draining vein showing > 50% thrombosis and multifocal aneurysms in draining vein. B. Inner wire of percutaneous thrombectomy device (PTD) kinked during thrombectomy for aneurysmal segment. C. Remnant PTD was removed through puncture site after cutting inner wire with wire cutters. D. Recanalization procedures were resumed with new PTD device. Flow was restored on completed fistulogram, despite residual thrombi.
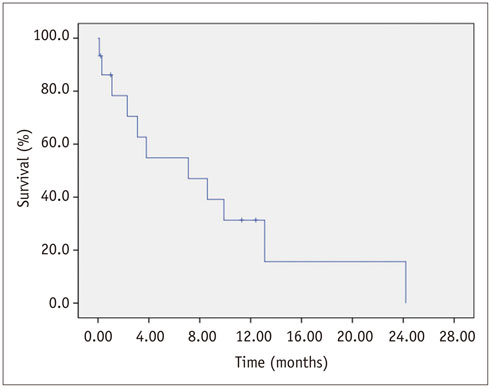
Fig. 3 Survival curve for primary patency after endovascular recanalization.
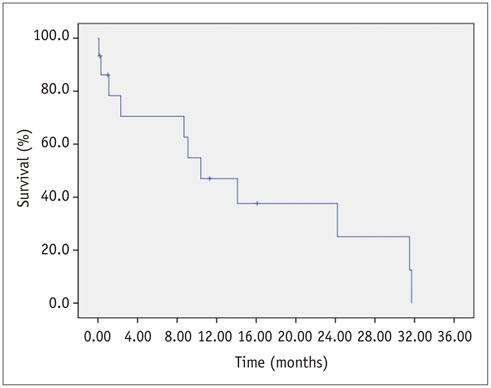
Fig. 4 Survival curve for secondary patency after endovascular recanalization.
Reference
-
1. Kalman PG, Pope M, Bhola C, Richardson R, Sniderman KW. A practical approach to vascular access for hemodialysis and predictors of success. J Vasc Surg. 1999; 30:727–733.2. NKF-DOQI clinical practice guidelines for vascular access. National Kidney Foundation-Dialysis Outcomes Quality Initiative. Am J Kidney Dis. 1997; 30:4 Suppl 3. S150–S191.3. Vascular Access 2006 Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006; 48:Suppl 1. S176–S247.4. Fan PY, Schwab SJ. Vascular access: concepts for the 1990s. J Am Soc Nephrol. 1992; 3:1–11.5. Joo SM, Kim HC, Min SI, Hur S, Jae HJ, Chung JW, et al. Recanalization of thrombosed arteriovenous fistulas for hemodialysis by minimal venotomy. J Vasc Interv Radiol. 2013; 24:401–405.6. Turmel-Rodrigues L. Application of percutaneous mechanical thrombectomy in autogenous fistulae. Tech Vasc Interv Radiol. 2003; 6:42–48.7. Won JH, Bista AB, Bae JI, Oh CK, Park SI, Lee JH, et al. A venotomy and manual propulsion technique to treat native arteriovenous fistulas occluded by thrombi. AJR Am J Roentgenol. 2012; 198:460–465.8. Bent CL, Sahni VA, Matson MB. The radiological management of the thrombosed arteriovenous dialysis fistula. Clin Radiol. 2011; 66:1–12.9. Hyun JH, Lee JH, Park SI. Hybrid surgery versus percutaneous mechanical thrombectomy for the thrombosed hemodialysis autogenous arteriovenous fistulas. J Korean Surg Soc. 2011; 81:43–49.10. Gray RJ, Sacks D, Martin LG, Trerotola SO. Society of Interventional Radiology Technology Assessment Committee. Reporting standards for percutaneous interventions in dialysis access. J Vasc Interv Radiol. 2003; 14(9 Pt 2):S433–S442.11. Salahi H, Fazelzadeh A, Mehdizadeh A, Razmkon A, Malek-Hosseini SA. Complications of arteriovenous fistula in dialysis patients. Transplant Proc. 2006; 38:1261–1264.12. Rajput A, Rajan DK, Simons ME, Sniderman KW, Jaskolka JD, Beecroft JR, et al. Venous aneurysms in autogenous hemodialysis fistulas: is there an association with venous outflow stenosis. J Vasc Access. 2013; 14:126–130.13. Pasklinsky G, Meisner RJ, Labropoulos N, Leon L, Gasparis AP, Landau D, et al. Management of true aneurysms of hemodialysis access fistulas. J Vasc Surg. 2011; 53:1291–1297.14. Bluestein D, Niu L, Schoephoerster RT, Dewanjee MK. Steady flow in an aneurysm model: correlation between fluid dynamics and blood platelet deposition. J Biomech Eng. 1996; 118:280–286.15. Peattie RA, Asbury CL, Bluth EI, Riehle TJ. Steady flow in models of abdominal aortic aneurysms. Part II: Wall stresses and their implication for in vivo thrombosis and rupture. J Ultrasound Med. 1996; 15:689–696.16. Rousseau H, Sapoval M, Ballini P, Dube M, Joffre F, Gaux JC, et al. Percutaneous recanalization of acutely thrombosed vessels by hydrodynamic thrombectomy (Hydrolyser). Eur Radiol. 1997; 7:935–941.17. Rajan DK, Clark TW, Simons ME, Kachura JR, Sniderman K. Procedural success and patency after percutaneous treatment of thrombosed autogenous arteriovenous dialysis fistulas. J Vasc Interv Radiol. 2002; 13:1211–1218.18. Shatsky JB, Berns JS, Clark TW, Kwak A, Tuite CM, Shlansky-Goldberg RD, et al. Single-center experience with the Arrow-Trerotola Percutaneous Thrombectomy Device in the management of thrombosed native dialysis fistulas. J Vasc Interv Radiol. 2005; 16:1605–1611.19. Cohen A, Korzets A, Neyman H, Ori Y, Baytner S, Belenky A, et al. Endovascular interventions of juxtaanastomotic stenoses and thromboses of hemodialysis arteriovenous fistulas. J Vasc Interv Radiol. 2009; 20:66–70.20. Cho SK, Han H, Kim SS, Lee JY, Shin SW, Do YS, et al. Percutaneous treatment of failed native dialysis fistulas: use of pulse-spray pharmacomechanical thrombolysis as the primary mode of therapy. Korean J Radiol. 2006; 7:180–186.21. Turmel-Rodrigues LA. Declotting a thrombosed Brescia-Cimino fistula by manual catheter-directed aspiration of the thrombus. Cardiovasc Intervent Radiol. 2005; 28:10–16.22. Rocek M, Peregrin JH, Lasovicková J, Krajícková D, Slavíoková M. Mechanical thrombolysis of thrombosed hemodialysis native fistulas with use of the Arrow-Trerotola percutaneous thrombolytic device: our preliminary experience. J Vasc Interv Radiol. 2000; 11:1153–1158.23. Vorwerk D, Schurmann K, Müller-Leisse C, Adam G, Bücker A, Sohn M, et al. Hydrodynamic thrombectomy of haemodialysis grafts and fistulae: results of 51 procedures. Nephrol Dial Transplant. 1996; 11:1058–1064.24. Sahni V, Kaniyur S, Malhotra A, Fan S, Blakeney C, Fotheringham T, et al. Mechanical thrombectomy of occluded hemodialysis native fistulas and grafts using a hydrodynamic thrombectomy catheter: preliminary experience. Cardiovasc Intervent Radiol. 2005; 28:714–721.25. Schmitz-Rode T, Wildberger JE, Hübner D, Wein B, Schürmann K, Günther RW. Recanalization of thrombosed dialysis access with use of a rotating mini-pigtail catheter: follow-up study. J Vasc Interv Radiol. 2000; 11:721–727.26. Kim HM, Kim HC, Woo S, Son KR, Jae HJ. Disconnection of the rubber tip of arrow-trerotola percutaneous thrombolytic device. Korean J Radiol. 2014; 15:254–257.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Aneurysmectomy and graft interposition for giant thrombosed proximal internal carotid artery aneurysm: Technical details
- The feasibility of surgical salvage of thrombosed arteriovenous fistula by an interventional nephrologist
- Recanalization of Totally Thrombosed Giant Aneurysm: Case Report
- Coil Embolization of Ruptured Thrombosed Distal Superior Cerebellar Artery Aneurysm: A Case Report
- Stereotactic radiosurgery for dural arteriovenous fistula
