A Case with Multiple Punched-out Lesions in the Skull and Generalized Fractures Associated with Steroid-induced Osteoporosis
- Affiliations
-
- 1Department of Internal Medicine, Division of Endocrinology and Metabolism, The Catholic University of Korea, Seoul, Korea. mikang@catholic.ac.kr
- KMID: 1975987
- DOI: http://doi.org/10.11005/jbm.2012.19.2.133
Abstract
- Steroid-induced osteoporosis is the most common cause of secondary osteoporosis and accounts for one-fifth of all osteoporosis cases. The fracture incidence under steroid may be as high as 50%. However, many patients do not undergo appropriate risk assessment and treatment before and after steroid exposure. We described a 56-year-old male patient with multiple punched-out lesions in skull unusually as well as vertebral, fibular, rib and humeral fractures during steroid use without proper management.
Figure
-
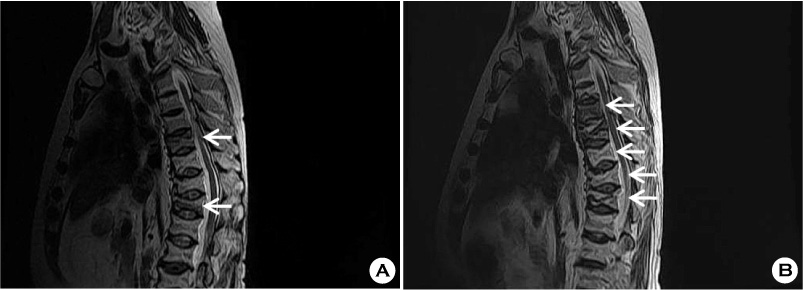
Fig. 1 (A) Six months ago, sagittal T2-weighted MRI of the thoracic spine showed acute compression fractures at T9 and T12. (B) After kyphoplasty, sagittal T2-weighted MRI of the lumbar spine showed acute compression fractures at T8, T10 and T11 and prominent fracture lines at T9 and T12.
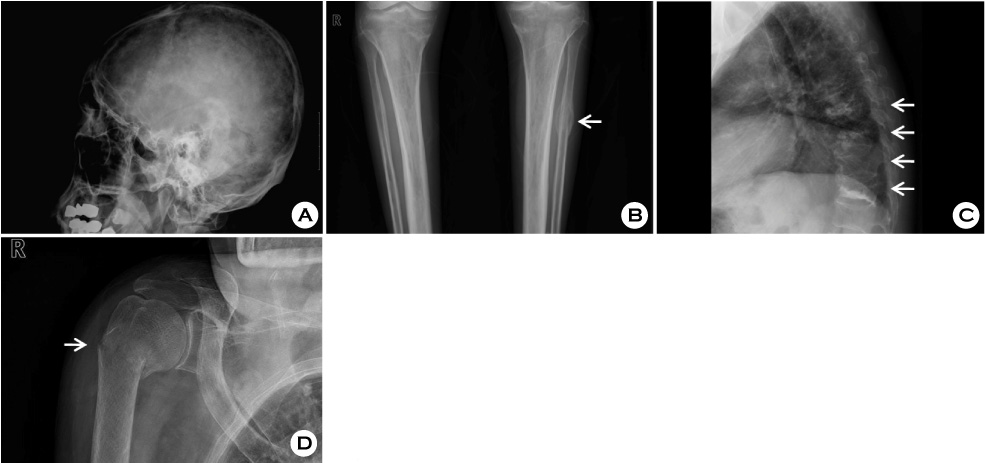
Fig. 2 (A) Lateral radiograph of the skull demonstrates multiple punched-out lesions with variable sizes on the parietal region. (B) Lateral radiograph of thoracic spine shows kyphosis of the thoracic vertebrae and multiple compression fractures with vertebroplasty segments at T8 through T12. (C) Posteroanterior plain radiograph demonstrates a left healed fibular fracture.
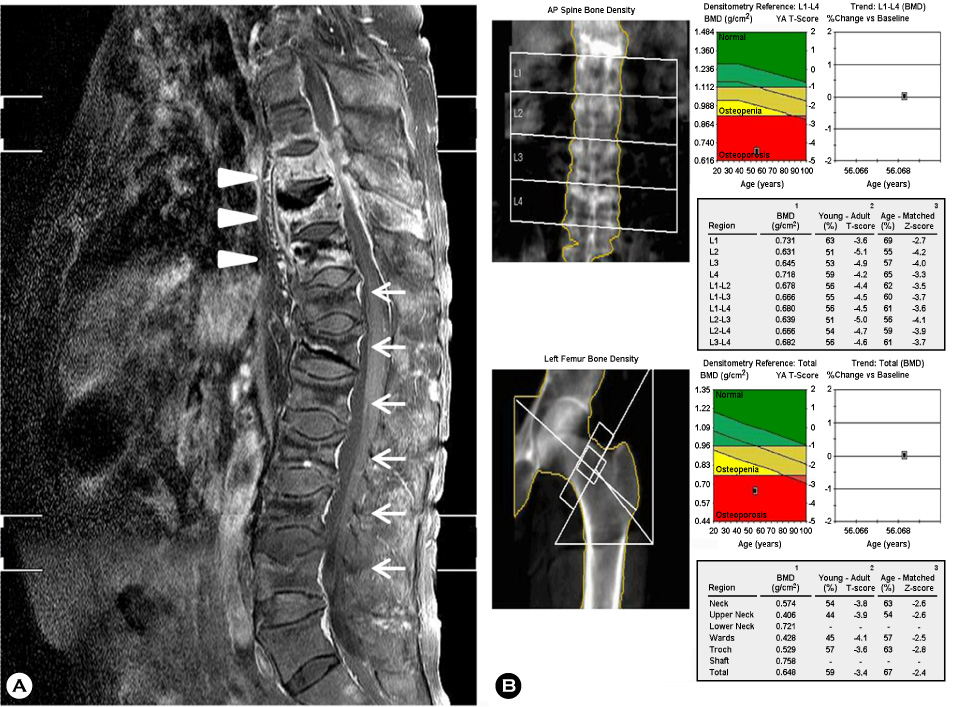
Fig. 3 (A) Sagittal fat-suppressed contrast-enhanced T2 weighted MRI of the spine shows spondylitis of T8, 9, 10 with left paraspinal and anterior subligamentous abscesses (arrow head) and compression fractures at T8 through L5. (B) Low bone mineral density at lumbar spine and left femur is demonstrated, indicating "osteoporosis". AP, anteroposterior; BMD, bone mineral density.
Reference
-
1. Mitra R. Adverse effects of corticosteroids on bone metabolism: a review. PM R. 2011. 3:466–471.
Article2. Weinstein RS. Clinical practice. Glucocorticoid-induced bone disease. N Engl J Med. 2011. 365:62–70.3. McDonough AK, Curtis JR, Saag KG. The epidemiology of glucocorticoid-associated adverse events. Curr Opin Rheumatol. 2008. 20:131–137.
Article4. Fitzpatrick LA. Secondary causes of osteoporosis. Mayo Clin Proc. 2002. 77:453–468.
Article5. Bogoch ER, Elliot-Gibson V, Wang RY, et al. Secondary causes of osteoporosis in fracture patients. J Orthop Trauma. 2012. 26:e145–e152.
Article6. van Staa TP, Leufkens HG, Cooper C. The epidemiology of corticosteroid-induced osteoporosis: a meta-analysis. Osteoporos Int. 2002. 13:777–787.
Article7. Grossman JM, Gordon R, Ranganath VK, et al. American College of Rheumatology 2010 recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res (Hoboken). 2010. 62:1515–1526.
Article8. Hardy R, Cooper MS. Adrenal gland and bone. Arch Biochem Biophys. 2010. 503:137–145.
Article9. Canalis E. Mechanisms of glucocorticoid-induced osteoporosis. Curr Opin Rheumatol. 2003. 15:454–457.
Article10. Avancini-Dobrović V, Vrbanić TS, Kukuljan M, et al. Spontaneous serial fractures of metatarsal bones in female patient with rheumatoid arthritis on long-term steroid therapy. Coll Antropol. 2010. 34:1123–1126.11. Lloyd ME, Davitt S, Hall JR. Bilateral tibia and fibula fractures in a patient with rheumatoid arthritis. Clin Rheumatol. 2001. 20:270–272.
Article12. Majumdar SR, Lix LM, Yogendran M, et al. Population-based trends in osteoporosis management after new initiations of long-term systemic glucocorticoids (1998-2008). J Clin Endocrinol Metab. 2012. 97:1236–1242.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical & radiological obstervations of multiple myeloma
- Tuberculous Periostitis of the Orbit: A Case Report
- A Case of Histiocytosis-X
- Vertebroplasty in the Multiple Osteoporotic Compression Fracture
- Long Term Use of Glucocorticoid Induced Osteoporotic Multiple Compression Fractures in Autoimmune Diseases
