A Mycotic Pulmonary Artery Aneurysm Associated with Candida Endocarditis: Case Report
- Affiliations
-
- 1Department of Radiology, Pusan National University School of Medicine, Medical Research Institute, Pusan National University Hospital, Busan, Korea.
- 2Department of Thoraci cand Cardiovascular Surgery, Pusan National University School of Medicine, Medical Research Institute, Pusan National University Hospital, Busan, Korea. song77.sh@gmail.com
- KMID: 1839433
- DOI: http://doi.org/10.3348/jksr.2014.70.3.205
Abstract
- We report a case of a mycotic pulmonary aneurysm associated with Candida endocarditis in a 53-year-old male with lymphoma. The initial diagnosis was a pulmonary artery aneurysm attributable to vasculitis, such as that associated with Behcet's disease, but a mycotic pulmonary artery aneurysm was later considered as a differential diagnosis. Identification of valve vegetation on the chest CT was helpful in this regard. We review the literature on the disease etiology, radiological findings, and management options.
MeSH Terms
Figure
-
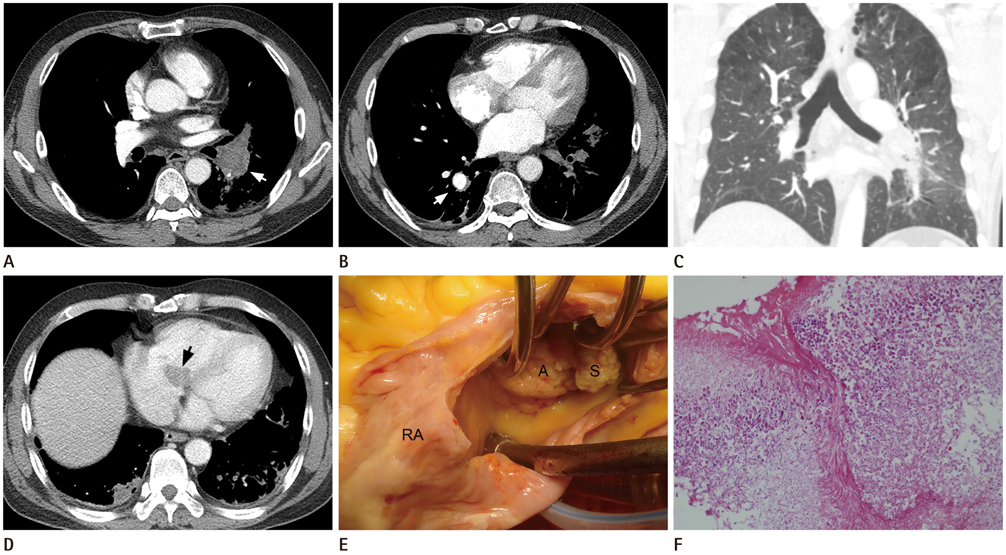
Fig. 1 A 53-year-old male patient diagnosed with mycotic pulmonary artery aneurysm associated with Candida endocarditis. A. An axial CT scan reveals an aneurysm with thrombus in the left inferior pulmonary artery (arrow). B. An axial scan taken a few centimeters below the level of scan (A) reveals an aneurysm of the right posterior basal segmental pulmonary artery (arrow). C. A coronal reformatted CT image at lung window setting shows no adjacent pneumonic consolidation or cavitary nodules in both lungs. D. Two weeks after follow-up CT reveals a low attenuated mass (arrow) at the right atrioventricular septum, which is suspected to be thrombus or vegetation. E. The surgical field contains large vegetations attached to the anterior (A) and septal (S) leaflets of the tricuspid valve. F. A photomicrograph showing abundant fungal hyphae in vegetation removed from the tricuspid valve, consistent with the presence of Candida species (hematoxylin-eosin staining; × 400).
Reference
-
1. Kim HS, Oh YW, Noh HJ, Lee KY, Kang EY, Lee SY. Mycotic pulmonary artery aneurysm as an unusual complication of thoracic actinomycosis. Korean J Radiol. 2004; 5:68–71.2. Müller KA, Zürn CS, Patrik H, Heuschmid M, Hetzel J, Henning A, et al. Massive haemoptysis in an intravenous drug user with infective tricuspid valve endocarditis. BMJ Case Rep. 2010; 2010.3. Navarro C, Dickinson PC, Kondlapoodi P, Hagstrom JW. Mycotic aneurysms of the pulmonary arteries in intravenous drug addicts. Report of three cases and review of the literature. Am J Med. 1984; 76:1124–1113.4. Prendergast BD, Tornos P. Surgery for infective endocarditis: who and when? Circulation. 2010; 121:1141–1152.5. International Study Group for Behçet's Disease. Criteria for diagnosis of Behçet's disease. Lancet. 1990; 335:1078–1080.6. Lee WK, Mossop PJ, Little AF, Fitt GJ, Vrazas JI, Hoang JK, et al. Infected (mycotic) aneurysms: spectrum of imaging appearances and management. Radiographics. 2008; 28:1853–1868.7. Sever M, Verstovsek S, Erasmus J Jr, Mattiuzzi GN. Mycotic pulmonary artery aneurysm due to Aspergillus infection in a patient with leukemia: case report and review of the literature. Leuk Res. 2010; 34:e133–e136.8. Choyke PL, Edmonds PR, Markowitz RI, Kleinman CS, Laks H. Mycotic pulmonary artery aneurysm: complication of Aspergillus endocarditis. AJR Am J Roentgenol. 1982; 138:1172–1175.9. Talwar S, Sharma R, Das B, Bhan A, Ray R, Saxena A, et al. Multiple fungal mycotic pulmonary artery aneurysms in an infant. Indian Heart J. 2000; 52:343–345.10. Roush K, Scala-Barnett DM, Donabedian H, Freimer EH. Rupture of a pulmonary artery mycotic aneurysm associated with candidal endocarditis. Am J Med. 1988; 84:142–144.11. Wijesekera NT, Sheppard MN, Mullen MJ. Candida endocarditis with mycotic pulmonary emboli following re-do Rastelli operation. Heart. 2004; 90:e34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coil Embolizaton of Mycotic Pulmonary Artery Aneurysm: A Case Report
- Infected Thoracic Aortic Aneurysm Concurrent with Endophthalmitis by Candida albicans: a Case Report
- A Case of Infective Endocarditis Complicated with Multiple Myocotic Aneurysm and Mitral Valve Perforation
- N-butyl Cyanoacrylate Embolization of Intracranial Mycotic Aneurysm: A Case Report
- A Case of Infective Bacterial Endocarditis Complicated by Acute Hemorrhagic Pericarditis and Hemoperitoneum by Rupture of Mycotic Aneurysm at Superior Mesenteric Artery
