A Case of Left Ventricular Noncompaction Accompanying Fasciculo-Ventricular Accessory Pathway and Atrial Flutter
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. clement@naver.com
- KMID: 1826469
- DOI: http://doi.org/10.4070/kcj.2012.42.10.705
Abstract
- Left ventricular hypertrabeculation/noncompaction (LVHT) is an uncommon type of genetic cardiomyopathy characterized by trabeculations and recesses within the ventricular myocardium. LVHT is associated with diastolic or systolic dysfunction, thromboembolic complications, and arrhythmias, including atrial fibrillation, ventricular arrhythmias, atrioventricular block and Wolff-Parkinson-White syndrome. Herein, we describe a patient who presented with heart failure and wide-complex tachycardia. Echocardiography showed LVHT accompanied with severe mitral regurgitation. The electrophysiologic study revealed a fasciculo-ventricular accessory pathway and atrial flutter (AFL). The AFL was successfully treated with catheter ablation.
Keyword
MeSH Terms
Figure
-

Fig. 1 The electrocardiography showed sinus rhythm, ventricular pre-excitation, and bizarre ST and T wave abnormality.

Fig. 2 The apical view of echocardiography (A) and cardiac magnetic resonance imaging (B) demonstrated deep trabeculations and recesses in the left ventricle.

Fig. 3 During the tachycardia, the heart rate was 140 beats per minute and the QRS morphology was similar to the sinus rhythm.
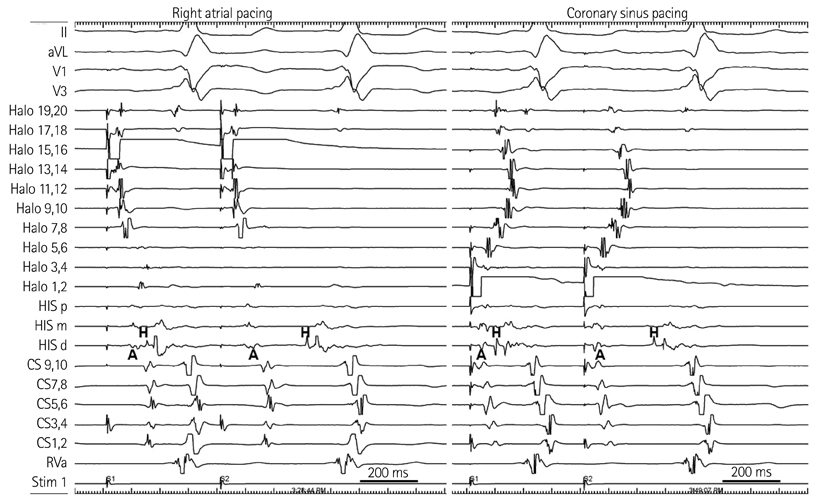
Fig. 4 Programmed atrial pacing from right atrium (left) and coronary sinus (right). A duodecapolar catheter was located in the right atrium (Halo). The S1 interval was 700 ms, which was followed by extrastimulus (S2) of 400 ms. Note that S2 caused prolongation of AH interval, but did not affect the HV interval. The HV interval and the degree of pre-excitation remained unchanged from both right atrial and coronary sinus pacing with atrial extrastimuli. CS: coronary sinus, RVa: right ventricular apex, AH: atrium to his, HV: his to ventricle.
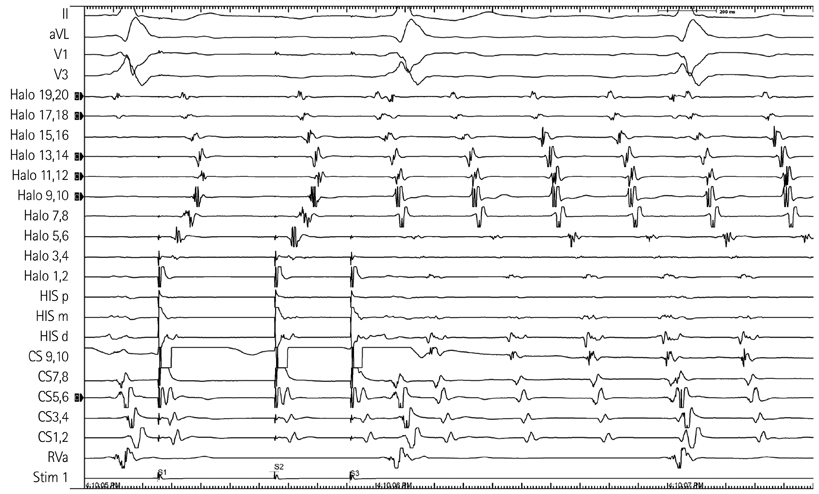
Fig. 5 Programmed atrial pacing on the proximal coronary sinus area induced typical atrial flutter. CS: coronary sinus, RVa: right ventricular apex.
Reference
-
1. Stöllberger C, Finsterer J. Arrhythmias and left ventricular hypertrabeculation/noncompaction. Curr Pharm Des. 2010. 16:2880–2894.2. Jenni R, Oechslin E, Schneider J, Attenhofer Jost C, Kaufmann PA. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001. 86:666–671.3. Sarma RJ, Chana A, Elkayam U. Left ventricular noncompaction. Prog Cardiovasc Dis. 2010. 52:264–273.4. Oechslin E, Jenni R. Left ventricular non-compaction revisited: a distinct phenotype with genetic heterogeneity? Eur Heart J. 2011. 32:1446–1456.5. Ichida F, Hamamichi Y, Miyawaki T, et al. Clinical features of isolated noncompaction of the ventricular myocardium: long-term clinical course, hemodynamic properties, and genetic background. J Am Coll Cardiol. 1999. 34:233–240.6. Sasse-Klaassen S, Gerull B, Oechslin E, Jenni R, Thierfelder L. Isolated noncompaction of the left ventricular myocardium in the adult is an autosomal dominant disorder in the majority of patients. Am J Med Genet A. 2003. 119A:162–167.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Mechanisms of Tachyarrhythmias in Infants with Structurally Normal Heart
- Stroke in a Young Individual with Left Ventricular Noncompaction and Left Atrium Standstill
- Noncompaction of Ventricular Myocardium Involving the Right Ventricle
- Atrial flutter associated with high pressure pneumoperitoneum during laparoscopic gastrectomy: A case report
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
