Anterior Atlantodental and Posterior Atlantodental Intervals on Plain Radiography, Multidetector CT, and MRI
- Affiliations
-
- 1Department of Radiology, Hanyang University Guri Hospital, Hanyang University College of Medicine, Guri, Korea. ryuja@hanyang.ac.kr
- 2Department of Radiology, Hanyang University Seoul Hospital, Hanyang University College of Medicine, Seoul, Korea.
- KMID: 1823935
- DOI: http://doi.org/10.3348/jksr.2015.72.1.57
Abstract
- PURPOSE
To determine the normal values of the anterior atlantodental interval (AADI) and posterior atlantodental interval (PADI) on plain radiography, multidetector CT (MDCT) and MRI, as well as the dural sac width and spinal cord diameter at the atlantoaxial joint level on MRI.
MATERIALS AND METHODS
In total, 60 subjects underwent plain radiography, MRI and MDCT. We obtained values for AADI and PADI on plain radiography, MDCT, and MRI, and for dural sac width and spinal cord diameter on MRI. Two radiologists independently measured each value and a consensus was reached.
RESULTS
The average AADI was 1.5 +/- 0.5 mm on plain radiography, 1.4 +/- 0.3 mm on MDCT, and 1.6 +/- 0.5 mm on MRI. The average PADI was 20.6 +/- 2.4 mm on plain radiography, 18.0 +/- 2.1 mm on MDCT, and 17.7 +/- 1.9 mm on MRI. The dural sac width was 13.7 +/- 1.8 mm, and the spinal cord diameter was 7.8 +/- 0.7 mm. Interobserver agreement was 0.701-0.927 and intraobserver agreement was 0.681-0.937.
CONCLUSION
AADI values obtained on MDCT are significantly lower than those obtained on plain radiography or MRI. PADI values obtained on plain radiography are significantly higher than those obtained on MDCT or MRI. The dural sac width is most closely correlated with PADI values on MDCT. PADI seems to be easier to measure, more relevant, and clinically useful than AADI.
MeSH Terms
Figure
-
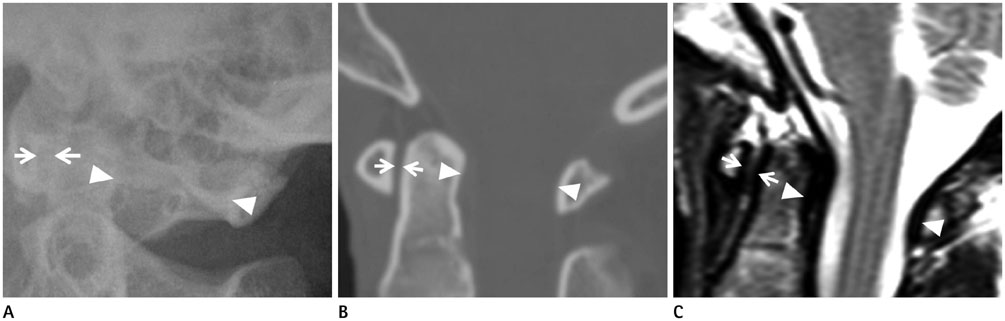
Fig. 1 Anterior atlantodental interval (AADI) and posterior atlantodental interval (PADI) on plain radiography, multidetector CT (MDCT), and MRI. A. A representative normal subject shows AADI (distance between white arrows) and PADI (distance between arrowheads) on plain radiography. B. A representative normal subject shows AADI (distance between white arrows) and PADI (distance between arrowheads) on MDCT. C. A representative normal subject shows AADI (distance between white arrows) and PADI (distance between arrowheads) on MRI.

Fig. 2 AADI on plain radiography, MDCT, and MRI. The differences and tendencies of the AADI values measured on plain radiography, MDCT, and MRI can be seen. AADI on MDCT is significantly below that on plain radiography and MRI (p < 0.05). Note.-AADI = anterior atlantodental interval, MDCT = multidetector CT, PL = plain radiography
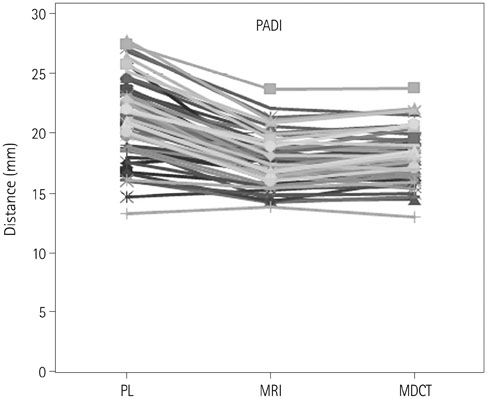
Fig. 3 PADI on plain radiography, MDCT, and MRI. The differences and tendencies of PADI values measured on plain radiography, MDCT, and MRI can be seen. PADI on plain radiography is significantly larger than on MDCT and MRI (p < 0.05). Note.-MDCT = multidetector CT, PADI = posterior atlantodental interval, PL = plain radiography
Reference
-
1. Patel AA, Spiker WR, Ghanayem AJ. Chapter 3. Functional anatomy of joints, ligaments, and discs. In : Benzel EC, editor. The Cervical spine. 5th ed. Philadelphia: Lippincott Williams & Wilkins/Wolters Kluwer;2012. p. 43–52.2. Schweitzer ME, Hodler J, Cervilla V, Resnick D. Craniovertebral junction: normal anatomy with MR correlation. AJR Am J Roentgenol. 1992; 158:1087–1090.3. Lee JS, Lee S, Bang SY, Choi KS, Joo KB, Kim YB, et al. Prevalence and risk factors of anterior atlantoaxial subluxation in ankylosing spondylitis. J Rheumatol. 2012; 39:2321–2326.4. Rojas CA, Bertozzi JC, Martinez CR, Whitlow J. Reassessment of the craniocervical junction: normal values on CT. AJNR Am J Neuroradiol. 2007; 28:1819–1823.5. Bertozzi JC, Rojas CA, Martinez CR. Evaluation of the pediatric craniocervical junction on MDCT. AJR Am J Roentgenol. 2009; 192:26–31.6. Coutts MB. Atlanto-epistropheal subluxations. Arch Surg. 1934; 29:297–311.7. Hinck VC, Hopkins CE. Measurement of the atlanto-dental interval in the adult. Am J Roentgenol Radium Ther Nucl Med. 1960; 84:945–951.8. Bundschuh C, Modic MT, Kearney F, Morris R, Deal C. Rheumatoid arthritis of the cervical spine: surface-coil MR imaging. AJR Am J Roentgenol. 1988; 151:181–187.9. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 1993; 75:1282–1297.10. Grauer JN, Tingstad EM, Rand N, Christie MJ, Hilibrand AS. Predictors of paralysis in the rheumatoid cervical spine in patients undergoing total joint arthroplasty. J Bone Joint Surg Am. 2004; 86-A:1420–1424.11. Yurube T, Sumi M, Nishida K, Miyamoto H, Kohyama K, Matsubara T, et al. Incidence and aggravation of cervical spine instabilities in rheumatoid arthritis: a prospective minimum 5-year follow-up study of patients initially without cervical involvement. Spine (Phila Pa 1976). 2012; 37:2136–2144.12. Kim DH, Hilibrand AS. Rheumatoid arthritis in the cervical spine. J Am Acad Orthop Surg. 2005; 13:463–474.13. Seo SJ, Kim HR, Choi EJ, Nahm FS. Unrecognized c1 lateral mass fracture without instability; the origin of posterior neck pain. Korean J Pain. 2012; 25:258–261.14. Harris J Jr. The cervicocranium: its radiographic assessment. Radiology. 2001; 218:337–351.15. Gale SC, Gracias VH, Reilly PM, Schwab CW. The inefficiency of plain radiography to evaluate the cervical spine after blunt trauma. J Trauma. 2005; 59:1121–1125.16. Diaz JJ Jr, Aulino JM, Collier B, Roman C, May AK, Miller RS, et al. The early work-up for isolated ligamentous injury of the cervical spine: does computed tomography scan have a role? J Trauma. 2005; 59:897–903. discussion 903-904.17. Simon JB, Schoenfeld AJ, Katz JN, Kamath A, Wood K, Bono CM, et al. Are "normal" multidetector computed tomographic scans sufficient to allow collar removal in the trauma patient? J Trauma. 2010; 68:103–108.18. Lee SL, Sena M, Greenholz SK, Fledderman M. A multidisciplinary approach to the development of a cervical spine clearance protocol: process, rationale, and initial results. J Pediatr Surg. 2003; 38:358–362. discussion 358-362.19. Radcliff K, Kepler C, Reitman C, Harrop J, Vaccaro A. CT and MRI-based diagnosis of craniocervical dislocations: the role of the occipitoatlantal ligament. Clin Orthop Relat Res. 2012; 470:1602–1613.20. Hogan GJ, Mirvis SE, Shanmuganathan K, Scalea TM. Exclusion of unstable cervical spine injury in obtunded patients with blunt trauma: is MR imaging needed when multi-detector row CT findings are normal? Radiology. 2005; 237:106–113.21. Muchow RD, Resnick DK, Abdel MP, Munoz A, Anderson PA. Magnetic resonance imaging (MRI) in the clearance of the cervical spine in blunt trauma: a meta-analysis. J Trauma. 2008; 64:179–189.22. Chen Y, Zhuang Z, Qi W, Yang H, Chen Z, Wang X, et al. A three-dimensional study of the atlantodental interval in a normal Chinese population using reformatted computed tomography. Surg Radiol Anat. 2011; 33:801–806.23. Osmotherly PG, Rivett DA, Rowe LJ. The anterior shear and distraction tests for craniocervical instability. An evaluation using magnetic resonance imaging. Man Ther. 2012; 17:416–421.24. Dvorak J, Grob D, Baumgartner H, Gschwend N, Grauer W, Larsson S. Functional evaluation of the spinal cord by magnetic resonance imaging in patients with rheumatoid arthritis and instability of upper cervical spine. Spine (Phila Pa 1976). 1989; 14:1057–1064.25. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979; 86:420–428.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sacroiliitis in Ankylosing Spondylitis: Comparison with Multidetector Row CT and Plain Radiography
- Unrecognized C1 Lateral Mass Fracture Without Instability; The Origin of Posterior Neck Pain
- Nonrheumatoid Retro-Odontoid Pseudotumors: Characteristics, Surgical Outcomes, and Time-Dependent Regression After Posterior Fixation
- Clinical Importance of MRI in Thoracolumbar Spinal Fracture
- Measurement Discrepancy of Sagittal Parameters between Plain Radiography and 3D Computed Tomography in Thoracolumbar and Lumbar Fractures
