J Korean Med Sci.
2014 Jun;29(6):776-781. 10.3346/jkms.2014.29.6.776.
Clinical Features of Right-Sided Infective Endocarditis Occurring in Non-Drug Users
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea.
- 2Division of Cardiology, Cardiac and Vascular Center, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. s.woo.park@samsung.com
- 3Division of Infectious Disease, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1796938
- DOI: http://doi.org/10.3346/jkms.2014.29.6.776
Abstract
- Right-sided infective endocarditis (RIE) occurs predominantly in intravenous drug users in western countries, and it has a relatively good prognosis. Clinical features and prognosis of RIE occurring in non-drug users are not well known. We investigated the clinical findings of RIE in non-drug users. We retrospectively reviewed 345 cases diagnosed with IE. Cases with RIE or left-sided infective endocarditis (LIE) defined by the vegetation site were included and cases having no vegetation or both-side vegetation were excluded. Clinical findings and in-hospital outcome of RIE were compared to those of LIE. Among the 245 cases, 39 (16%) cases had RIE and 206 (84%) cases had LIE. RIE patients were younger (40+/-19 yr vs 50+/-18 yr, P=0.004), and had a higher incidence of congenital heart disease (CHD) (36% vs 13%, P<0.001) and central venous catheter (CVC) (21% vs 4%, P=0.001) compared to LIE patients. A large vegetation was more common in RIE (33% vs 9%, P<0.001). Staphylococcus aureus was the most common cause of RIE, while Streptococcus viridans were the most common cause of LIE. In-hospital mortality and cardiac surgery were not different between the two groups. CHD and use of CVC were common in non-drug users with RIE. The short-term clinical outcome of RIE is not different from that of LIE.
Keyword
MeSH Terms
-
Adult
Aged
Central Venous Catheters/microbiology
Echocardiography
Endocarditis, Bacterial/*diagnosis/microbiology/mortality
Female
Heart Defects, Congenital/complications/epidemiology
Hospital Mortality
Humans
Incidence
Male
Middle Aged
Prognosis
Retrospective Studies
Staphylococcus aureus/isolation & purification
Viridans Streptococci/isolation & purification
Young Adult
Figure
-
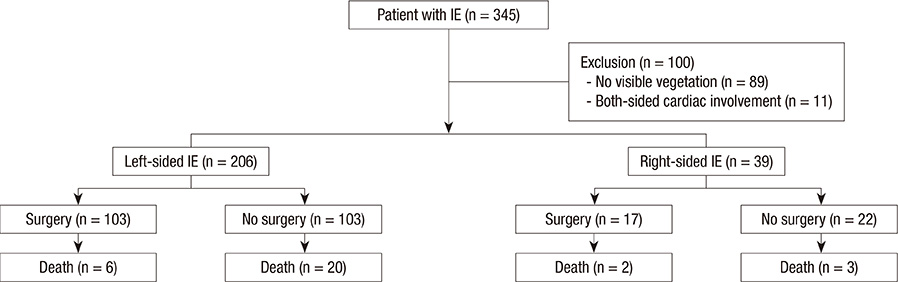
Fig. 1 Flow diagram of the study population and the outcome in 245 cases of right-sided infective endocarditis (IE) and left-sided IE.
Reference
-
1. Chan P, Ogilby JD, Segal B. Tricuspid valve endocarditis. Am Heart J. 1989; 117:1140–1146.2. Hecht SR, Berger M. Right-sided endocarditis in intravenous drug users. Prognostic features in 102 episodes. Ann Intern Med. 1992; 117:560–566.3. Sutcliffe EC, Terasaki GS, Thompson RE. Tricuspid endocarditis with pulmonary emboli. Respir Care. 2006; 51:1471–1474.4. Mathew J, Addai T, Anand A, Morrobel A, Maheshwari P, Freels S. Clinical features, site of involvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch Intern Med. 1995; 155:1641–1648.5. Mathura KC, Thapa N, Rauniyar A, Magar A, Gurubacharya DL, Karki DB. Injection drug use and tricuspid valve endocarditis. Kathmandu Univ Med J (KUMJ). 2005; 3:84–86.6. Moss R, Munt B. Injection drug use and right sided endocarditis. Heart. 2003; 89:577–581.7. Martín-Dávila P, Navas E, Fortún J, Moya JL, Cobo J, Pintado V, Quereda C, Jiménez-Mena M, Moreno S. Analysis of mortality and risk factors associated with native valve endocarditis in drug users: the importance of vegetation size. Am Heart J. 2005; 150:1099–1106.8. Thalme A, Westling K, Julander I. In-hospital and long-term mortality in infective endocarditis in injecting drug users compared to non-drug users: a retrospective study of 192 episodes. Scand J Infect Dis. 2007; 39:197–204.9. Carozza A, De Santo LS, Romano G, Della Corte A, Ursomando F, Scardone M, Caianiello G, Cotrufo M. Infective endocarditis in intravenous drug abusers: patterns of presentation and long-term outcomes of surgical treatment. J Heart Valve Dis. 2006; 15:125–131.10. Miró JM, Moreno A, Mestres CA. Infective endocarditis in intravenous drug abusers. Curr Infect Dis Rep. 2003; 5:307–316.11. Cecchi E, Imazio M, Tidu M, Forno D, De Rosa FG, Dal Conte I, Preziosi C, Lipani F, Trinchero R. Infective endocarditis in drug addicts: role of HIV infection and the diagnostic accuracy of Duke criteria. J Cardiovasc Med (Hagerstown). 2007; 8:169–175.12. Schroeder RA. Pulmonic valve endocarditis in a normal heart. J Am Soc Echocardiogr. 2005; 18:197–198.13. Heydari AA, Safari H, Sarvghad MR. Isolated tricuspid valve endocarditis. Int J Infect Dis. 2009; 13:e109–e111.14. Kovarik A, Setina M, Sulda M, Pazderkova P, Mokracek A. Infective endocarditis of the tricuspid valve caused by Staphylococcus aureus after ear piercing. Scand J Infect Dis. 2007; 39:266–268.15. Bilen E, Yasar AS, Bilge M, Kurt M, Karakas F, Aslantas U. Isolated pulmonic valve endocarditis in an adult patient with ventricular septal defect and infundibular pulmonary stenosis. Echocardiography. 2008; 25:904–907.16. Hamza N, Ortiz J, Bonomo RA. Isolated pulmonic valve infective endocarditis: a persistent challenge. Infection. 2004; 32:170–175.17. Shimoni Z, Pitlik S, Szyper-Kravitz M, Sagie A, Bishara J. Tricuspid valve endocarditis in adult patients without known predisposing factors. Eur J Clin Microbiol Infect Dis. 2001; 20:49–51.18. Turhan O, Saba R, Belgi A, Inan D, Karaoglan H, Yalcin AN. A case of right-side infective endocarditis with ventricular septal defect. Infez Med. 2005; 13:39–41.19. Vaideeswar P, Jawale RM, Tullu M. Isolated infective endocarditis of the pulmonary valve: an autopsy analysis of nine cases. Cardiovasc Pathol. 2009; 18:231–235.20. Anguita Sánchez M, Torres Calvo F, Castillo Domínguez JC, Delgado Ortega M, Mesa Rubio D, Ruiz Ortiz M, Romo Peña E, Arizón del Prado JM, Suárez de Lezo J. Short- and long-term prognosis of infective endocarditis in non-injection drug users: improved results over 15 years (1987-2001). Rev Esp Cardiol. 2005; 58:1188–1196.21. Cecchi E, Forno D, Imazio M, Migliardi A, Gnavi R, Dal Conte I, Trinchero R. Piemonte Infective Endocarditis Study Group. New trends in the epidemiological and clinical features of infective endocarditis: results of a multicenter prospective study. Ital Heart J. 2004; 5:249–256.22. Hoen B, Alla F, Selton-Suty C, Béguinot I, Bouvet A, Briançon S, Casalta JP, Danchin N, Delahaye F, Etienne J, et al. Changing profile of infective endocarditis: results of a 1-year survey in France. JAMA. 2002; 288:75–81.23. Kim DH, Kang DH, Lee MZ, Yun SC, Kim YJ, Song JM, Song JK, Lee JW, Sohn DW. Impact of early surgery on embolic events in patients with infective endocarditis. Circulation. 2010; 122:S17–S22.24. Kang DH, Kim YJ, Kim SH, Sun BJ, Kim DH, Yun SC, Song JM, Choo SJ, Chung CH, Song JK, et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012; 366:2466–2473.25. Miró JM, del Río A, Mestres CA. Infective endocarditis in intravenous drug abusers and HIV-1 infected patients. Infect Dis Clin North Am. 2002; 16:273–295. vii–viii.26. Sandre RM, Shafran SD. Infective endocarditis: review of 135 cases over 9 years. Clin Infect Dis. 1996; 22:276–286.27. Siddiq S, Missri J, Silverman DI. Endocarditis in an urban hospital in the 1990s. Arch Intern Med. 1996; 156:2454–2458.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Active Infective Endocarditis with Vegetation of Right Atrium in Patient with End-stage Renal Disease
- A Case of Tricuspid Valve Endocarditis with Pulmonary Embolism in a Drug Addict
- A Case of Infective Endocarditis in which Cerebral Infarction and Hemorrhage developed together
- A Case of Tricuspid Valve Endocarditis with Vegetation in a Non-Drug Addict without Underlying Cardiac Disease
- Clinical and Echocardiographic Features of Pulmonic Valve Endocarditis in patients with Ventricular Septal Defect
