Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Affiliations
-
- 1Department of Neurology, Seoul National University College of Medicine, Seoul, Korea. kwoo@plaza.snu.ac.kr
- 2Department of Neurology, Hanyang University College of Medicine, Seoul, Korea.
- 3Department of Neurology, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1793038
- DOI: http://doi.org/10.3346/jkms.2013.28.9.1261
Abstract
- The recent developments of new devices and advances in anesthesiology have greatly improved the utility and accuracy of intraoperative neurophysiological monitoring (IOM). Herein, we review the basic principles of the electrophysiological methods employed under IOM in the operating room. These include motor evoked potentials, somatosensory evoked potentials, electroencephalography, electromyography, brainstem auditory evoked potentials, and visual evoked potentials. Most of these techniques have certain limitations and their utility is still being debated. In this review, we also discuss the optimal stimulation/recording method for each of these modalities during individual surgeries as well as the diverse criteria for alarm signs.
MeSH Terms
Figure
-
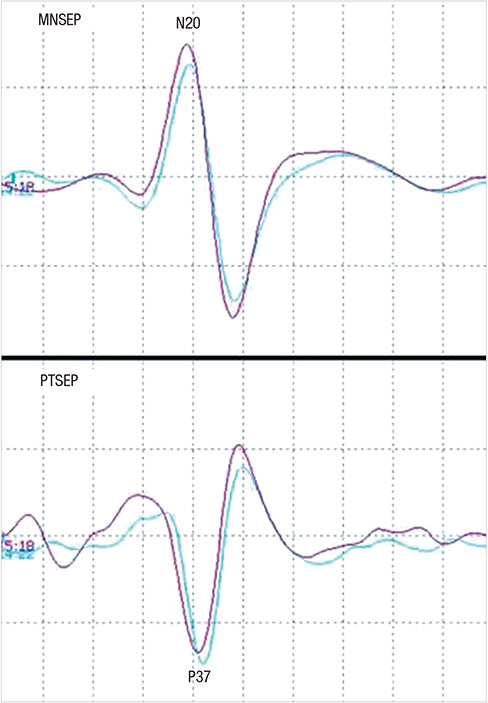
Fig. 1 Waves of median nerve somstosensory evoked potential (MNSEP) and posterior tibial nerve somatosensory evoked potential (PTSEP). Electrical stimulation at the median nerve and posterior tibial nerve can evoke generation of the cortical waves of N20 and P37, respectively.
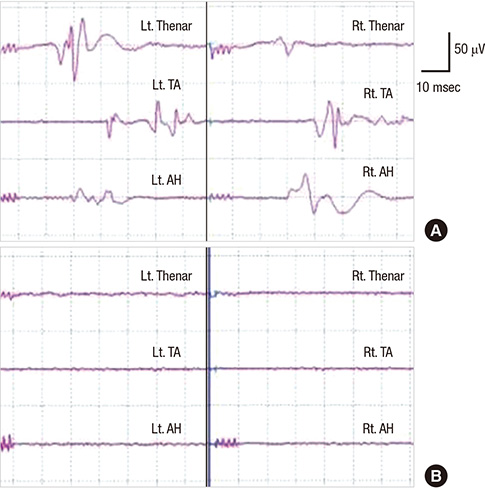
Fig. 2 Halogenated anesthetics can abolish the generation of motor evoked potential (MEP). MEP is generated well in a patient underwent surgery with total venous anesthesia (A). The MEP in this patient completely disappears on using halogenated gas anesthetics (B). This patient had no post-operative neural deficit.

Fig. 3 Train of four (TOF) can monitor the degree of neuromuscular blockage in IOM with muscle motor evoked potential (mMEP). Both number and amplitude of muscle twitch, obtained with four consecutive electrical stimulation at the motor nerve (TOF), represent the degree of neuromuscular blockage. No muscle twitch is observed with the TOF and no mMEP are generated (A). When 4 muscle twitches were observed with TOF but the amplitude fourth muscle twitch (T4) were relative small, compared with that of first muscle twitch (T1), mMEP with small amplitude are generated (B). When four muscle twitches with constant amplitude are observed with TOF, mMEP with large amplitude are observed (C).

Fig. 4 Monitoring for the recurrent laryngeal nerve injury in thyroid surgery. During thyroidectomy, compound muscle action potential (CMAP) is recorded at the vocal cord muscles, using continuous nerve stimulation technique (A). The CMAP is abruptly lost during surgery and does not recover at the end of surgery (B). This patient experienced post-operative complication of the vocal cord paralysis.
Cited by 3 articles
-
Intraoperative monitoring of somatosensory and visual evoked potentials for detecting posterior cerebral artery infarction during anteromesial temporal resection
Suyeon Seo, Dong Jun Kim, Chae Young Lee
Ann Clin Neurophysiol. 2020;22(2):104-108. doi: 10.14253/acn.2020.22.2.104.Clinical Usefulness of Intraoperative Motor-Evoked Potential Monitoring during Temporal Lobe Epilepsy Surgery
Dae Lim Koo, Won Gu Lee, Seung-Chyul Hong, Dae-Won Seo
J Clin Neurol. 2019;15(3):285-291. doi: 10.3988/jcn.2019.15.3.285.Intraoperative monitoring of cortico-cortical evoked potentials of the frontal aslant tract in a patient with oligodendroglioma
Ha-rin Yang, Young-Shin Ra, Yong Seo Koo
Ann Clin Neurophysiol. 2022;24(1):21-25. doi: 10.14253/acn.2022.24.1.21.
Reference
-
1. Penfield W, Boldrey E. Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain. 1937; 60:389–443.2. Nuwer MR. Intraoperative monitoring of neural function. Amsterdam: Elsevier;2008.3. Kothbauer K, Deletis V, Epstein FJ. Intraoperative spinal cord monitoring for intramedullary surgery: an essential adjunct. Pediatr Neurosurg. 1997; 26:247–254.4. Kothbauer KF, Deletis V, Epstein FJ. Motor-evoked potential monitoring for intramedullary spinal cord tumor surgery: correlation of clinical and neurophysiological data in a series of 100 consecutive procedures. Neurosurg Focus. 1998; 4:e1.5. Greiner A, Mess WH, Schmidli J, Debus ES, Grommes J, Dick F, Jacobs MJ. Cyber medicine enables remote neuromonitoring during aortic surgery. J Vasc Surg. 2012; 55:1227–1232.6. Sloan TB, Heyer EJ. Anesthesia for intraoperative neurophysiologic monitoring of the spinal cord. J Clin Neurophysiol. 2002; 19:430–443.7. Rohde V, Krombach GA, Baumert JH, Kreitschmann-Andermahr I, Weinzierl M, Gilsbach JM. Measurement of motor evoked potentials following repetitive magnetic motor cortex stimulation during isoflurane or propofol anaesthesia. Br J Anaesth. 2003; 91:487–492.8. Kalkman CJ, Ubags LH, Been HD, Swaan A, Drummond JC. Improved amplitude of myogenic motor evoked responses after paired transcranial electrical stimulation during sufentanil/nitrous oxide anesthesia. Anesthesiology. 1995; 83:270–276.9. Calancie B, Harris W, Broton JG, Alexeeva N, Green BA. "Threshold-level" multipulse transcranial electrical stimulation of motor cortex for intraoperative monitoring of spinal motor tracts: description of method and comparison to somatosensory evoked potential monitoring. J Neurosurg. 1998; 88:457–470.10. Woodforth IJ, Hicks RG, Crawford MR, Stephen JP, Burke DJ. Variability of motor-evoked potentials recorded during nitrous oxide anesthesia from the tibialis anterior muscle after transcranial electrical stimulation. Anesth Analg. 1996; 82:744–749.11. Jacobs MJ, Meylaerts SA, de Haan P, de Mol BA, Kalkman CJ. Strategies to prevent neurologic deficit based on motor-evoked potentials in type I and II thoracoabdominal aortic aneurysm repair. J Vasc Surg. 1999; 29:48–57.12. Calancie B, Molano MR. Alarm criteria for motor-evoked potentials: what's wrong with the "presence-or-absence" approach? Spine (Phila Pa 1976). 2008; 33:406–414.13. Szelényi A, Hattingen E, Weidauer S, Seifert V, Ziemann U. Intraoperative motor evoked potential alteration in intracranial tumor surgery and its relation to signal alteration in postoperative magnetic resonance imaging. Neurosurgery. 2010; 67:302–313.14. Deletis V, Sala F. Intraoperative neurophysiological monitoring of the spinal cord during spinal cord and spine surgery: a review focus on the corticospinal tracts. Clin Neurophysiol. 2008; 119:248–264.15. Kim SM, Yang H, Park SB, Han SG, Park KW, Yoon SH, Hyun SJ, Kim HJ, Park KS, Lee KW. Pattern-specific changes and discordant prognostic values of individual leg-muscle motor evoked potentials during spinal surgery. Clin Neurophysiol. 2012; 123:1465–1470.16. Jankowska E, Padel Y, Tanaka R. Projections of pyramidal tract cells to alpha-motoneurones innervating hind-limb muscles in the monkey. J Physiol. 1975; 249:637–667.17. Ulkatan S, Neuwirth M, Bitan F, Minardi C, Kokoszka A, Deletis V. Monitoring of scoliosis surgery with epidurally recorded motor evoked potentials (D wave) revealed false results. Clin Neurophysiol. 2006; 117:2093–2101.18. Dong CC, MacDonald DB, Janusz MT. Intraoperative spinal cord monitoring during descending thoracic and thoracoabdominal aneurysm surgery. Ann Thorac Surg. 2002; 74:S1873–S1876.19. Dinner DS, Lüders H, Lesser RP, Morris HH, Barnett G, Klem G. Intraoperative spinal somatosensory evoked potential monitoring. J Neurosurg. 1986; 65:807–814.20. Nuwer MR, Dawson EG, Carlson LG, Kanim LE, Sherman JE. Somatosensory evoked potential spinal cord monitoring reduces neurologic deficits after scoliosis surgery: results of a large multicenter survey. Electroencephalogr Clin Neurophysiol. 1995; 96:6–11.21. Thompson JE. Surgery for cerebrovascular insufficiency (stroke) with special emphasis on carotid endarterectomy. Springfield: Thomas;1968.22. Rampil IJ. A primer for EEG signal processing in anesthesia. Anesthesiology. 1998; 89:980–1002.23. Akiyama T, Kobayashi K, Nakahori T, Yoshinaga H, Ogino T, Ohtsuka Y, Takeuchi M, Morita K, Sano S, Oka E. Electroencephalographic changes and their regional differences during pediatric cardiovascular surgery with hypothermia. Brain Dev. 2001; 23:115–121.24. Jansen C, Moll FL, Vermeulen FE, van Haelst JM, Ackerstaff RG. Continuous transcranial Doppler ultrasonography and electroencephalography during carotid endarterectomy: a multimodal monitoring system to detect intraoperative ischemia. Ann Vasc Surg. 1993; 7:95–101.25. Martin CJ, Sinson G, Patterson T, Zager EL, Stecker MM. Sensitivity of scalp EEG, cortical EGG, and somatosensory evoked responses during surgery for intracranial aneurysms. Surg Neurol. 2002; 58:317–320.26. Harper CM, Daube JR. Facial nerve electromyography and other cranial nerve monitoring. J Clin Neurophysiol. 1998; 15:206–216.27. Prass RL, Lüders H. Acoustic (loudspeaker) facial electromyographic monitoring: part 1. evoked electromyographic activity during acoustic neuroma resection. Neurosurgery. 1986; 19:392–400.28. Yingling CD, Ashram YA. Intraoperative monitoring of cranial nerves in skull base surgery. In : Jackler RK, Brackmann DE, editors. Neurotology. 2nd ed. Philadelphia: Elsevier Mosby;2005.29. Grundy BL, Jannetta PJ, Procopio PT, Lina A, Boston JR, Doyle E. Intraoperative monitoring of brain-stem auditory evoked potentials. J Neurosurg. 1982; 57:674–681.30. Watanabe E, Schramm J, Strauss C, Fahlbusch R. Neurophysiologic monitoring in posterior fossa surgery: II. BAEP-waves I and V and preservation of hearing. Acta Neurochir (Wien). 1989; 98:118–128.31. James ML, Husain AM. Brainstem auditory evoked potential monitoring: when is change in wave V significant? Neurology. 2005; 65:1551–1555.32. Kodama K, Goto T, Sato A, Sakai K, Tanaka Y, Hongo K. Standard and limitation of intraoperative monitoring of the visual evoked potential. Acta Neurochir (Wien). 2010; 152:643–648.33. Sasaki T, Itakura T, Suzuki K, Kasuya H, Munakata R, Muramatsu H, Ichikawa T, Sato T, Endo Y, Sakuma J, et al. Intraoperative monitoring of visual evoked potential: introduction of a clinically useful method. J Neurosurg. 2010; 112:273–284.34. Torres CV, Pastor J, Rocío E, Sola RG. Continuous monitoring of cortical visual evoked potentials by means of subdural electrodes in surgery on the posterior optic pathway: a case report and review of the literature. Rev Neurol. 2012; 55:343–348.35. Chung SB, Park CW, Seo DW, Kong DS, Park SK. Intraoperative visual evoked potential has no association with postoperative visual outcomes in transsphenoidal surgery. Acta Neurochir (Wien). 2012; 154:1505–1510.36. American Association of Neuromuscular and Electrodiagnostic Medicine. AANEM POSITION STATEMENT: the role of the intraoperative monitoring team. accessed on 16 September 2008. Available at http://www.aanem.org/getmedia/44fbb8e3-27db-44e8-90df-81797109be2f/IOMMonitoringTeam_000.pdf.aspx.37. Health Care Financing Administration. Physician supervision of diagnostic tests. accessed on 19 April 2001. Available at http://www.aarc.org/members_area/advocacy/federal/md_supervision_tests.pdf.38. Nuwer JM, Nuwer MR. Neurophysiologic surgical monitoring staffing patterns in the USA. Electroencephalogr Clin Neurophysiol. 1997; 103:616–620.39. American Academy of Neurology. Principles of Coding for Intraoperative Neurophysiologic Monitoring (IOM) and Testing Model Policy. accessed on 10 February 2012. Available at http://www.aan.com/uploadedFiles/Website_Library_Assets/Documents/3.Practice_Management/1.Reimbursement/1.Billing_and_Coding/5.Coverage_Policies/Coverage%20Policies%20-%20IONM.pdf.40. Emerson R. Remote monitoring. In : Husain AM, editor. A practical approach to neurophysiologic intraoperative monitoring. New York: Demos;2008.41. Scheufler KM, Zentner J. Total intravenous anesthesia for intraoperative monitoring of the motor pathways: an integral view combining clinical and experimental data. J Neurosurg. 2002; 96:571–579.42. Huotari AM, Koskinen M, Suominen K, Alahuhta S, Remes R, Hartikainen KM, Jäntti V. Evoked EEG patterns during burst suppression with propofol. Br J Anaesth. 2004; 92:18–24.43. Schubert A, Licina MG, Lineberry PJ. The effect of ketamine on human somatosensory evoked potentials and its modification by nitrous oxide. Anesthesiology. 1990; 72:33–39.44. Ojemann G, Ojemann J, Lettich E, Berger M. Cortical language localization in left, dominant hemisphere: an electrical stimulation mapping investigation in 117 patients. J Neurosurg. 1989; 71:316–326.45. Duffau H. Lessons from brain mapping in surgery for low-grade glioma: insights into associations between tumour and brain plasticity. Lancet Neurol. 2005; 4:476–486.46. Møller AR. Intraoperative neurophysiologic monitoring. United Kingdom: Harwood Academic;1995.47. Randolph GW, Dralle H, Abdullah H, Barczynski M, Bellantone R, Brauckhoff M, Carnaille B, Cherenko S, Chiang FY, Dionigi G, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011; 121:S1–S16.48. Brennan J, Moore EJ, Shuler KJ. Prospective analysis of the efficacy of continuous intraoperative nerve monitoring during thyroidectomy, parathyroidectomy, and parotidectomy. Otolaryngol Head Neck Surg. 2001; 124:537–543.49. Neves DO, Lefaucheur JP, de Andrade DC, Hattou M, Ahdab R, Ayache SS, Le Guerinel C, Keravel Y. A reappraisal of the value of lateral spread response monitoring in the treatment of hemifacial spasm by microvascular decompression. J Neurol Neurosurg Psychiatry. 2009; 80:1375–1380.50. Ishikawa M, Ohira T, Namiki J, Ajimi Y, Takase M, Toya S. Abnormal muscle response (lateral spread) and F-wave in patients with hemifacial spasm. J Neurol Sci. 1996; 137:109–116.51. Kong DS, Park K, Shin BG, Lee JA, Eum DO. Prognostic value of the lateral spread response for intraoperative electromyography monitoring of the facial musculature during microvascular decompression for hemifacial spasm. J Neurosurg. 2007; 106:384–387.52. Nuwer MR, Emerson RG, Galloway G, Legatt AD, Lopez J, Minahan R, Yamada T, Goodin DS, Armon C, Chaudhry V, et al. Evidence-based guideline update: intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked potentials: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology. 2012; 78:585–589.53. Ovadia D, Korn A, Fishkin M, Steinberg DM, Wientroub S, Ofiram E. The contribution of an electronic conductivity device to the safety of pedicle screw insertion in scoliosis surgery. Spine (Phila Pa 1976). 2011; 36:E1314–E1321.54. Glassman SD, Dimar JR, Puno RM, Johnson JR, Shields CB, Linden RD. A prospective analysis of intraoperative electromyographic monitoring of pedicle screw placement with computed tomographic scan confirmation. Spine (Phila Pa 1976). 1995; 20:1375–1379.55. Guérit JM, Witdoeckt C, de Tourtchaninoff M, Ghariani S, Matta A, Dion R, Verhelst R. Somatosensory evoked potential monitoring in carotid surgery: I. relationships between qualitative SEP alterations and intraoperative events. Electroencephalogr Clin Neurophysiol. 1997; 104:459–469.56. Ackerstaff RG, Moons KG, van de Vlasakker CJ, Moll FL, Vermeulen FE, Algra A, Spencer MP. Association of intraoperative transcranial doppler monitoring variables with stroke from carotid endarterectomy. Stroke. 2000; 31:1817–1823.57. Thomusch O, Sekulla C, Machens A, Neumann HJ, Timmermann W, Dralle H. Validity of intra-operative neuromonitoring signals in thyroid surgery. Langenbecks Arch Surg. 2004; 389:499–503.58. Barczyński M, Konturek A, Cichoń S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg. 2009; 96:240–246.59. Friedrich C, Ulmer C, Rieber F, Kern E, Kohler A, Schymik K, Thon KP, Lamadé W. Safety analysis of vagal nerve stimulation for continuous nerve monitoring during thyroid surgery. Laryngoscope. 2012; 122:1979–1987.60. Zhong D, Zhou Y, Li Y, Wang Y, Zhou W, Cheng Q, Chen L, Zhao J, Li X, Yan X. Intraoperative recurrent laryngeal nerve monitoring: a useful method for patients with esophageal cancer. Dis Esophagus. 2012; doi: 10.1111/j.1442-2050.2012.01414.x.61. Kwok K, Davis B, Kliot M. Resection of a benign brachial plexus nerve sheath tumor using intraoperative electrophysiological monitoring. Neurosurgery. 2007; 60:316–320.62. Hickey C, Gugino LD, Aglio LS, Mark JB, Son SL, Maddi R. Intraoperative somatosensory evoked potential monitoring predicts peripheral nerve injury during cardiac surgery. Anesthesiology. 1993; 78:29–35.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical practice guidelines for intraoperative neurophysiological monitoring: 2020 update
- Intraoperative Neurophysiologic Monitoring and Functional Outcome in Cerebellopontine Angle Tumor Surgery
- Mechanisms underlying brain monitoring during anesthesia: limitations, possible improvements, and perspectives
- General Principles in Hemodynamic Monitoring
- Traumatic Brachial Plexus Injury: Preoperative Evaluation and Treatment Principles
