Tuberculous Pericarditis Presenting as Multiple Free Floating Masses in Pericardial Effusion
- Affiliations
-
- 1Department of Pediatrics, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. hshan@chungbuk.ac.kr
- 2Department of Thoracic and Cardiovascular Surgery, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea.
- 3Department of Pathology, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 1793007
- DOI: http://doi.org/10.3346/jkms.2012.27.3.325
Abstract
- Pericarditis is a rare manifestation of tuberculosis (Tb) in children. A 14-yr-old Korean boy presented with cardiac tamponade during treatment of pulmonary tuberculosis. He developed worsening anemia and persistent fever in spite of anti-tuberculosis medications. Echocardiography found free floating multiple discoid masses in the pericardial effusion. The masses and exudates were removed by pericardiostomy. The masses were composed of pink, amorphous meshwork of threads admixed with degenerated red blood cells and leukocytes with numerous acid-fast bacilli, which were confirmed as Mycobacterium species by polymerase chain reaction. The persistent fever and anemia were controlled after pericardiostomy. This is the report of a unique manifestation of Tb pericarditis as free floating masses in the effusion with impending tamponade.
MeSH Terms
Figure
-
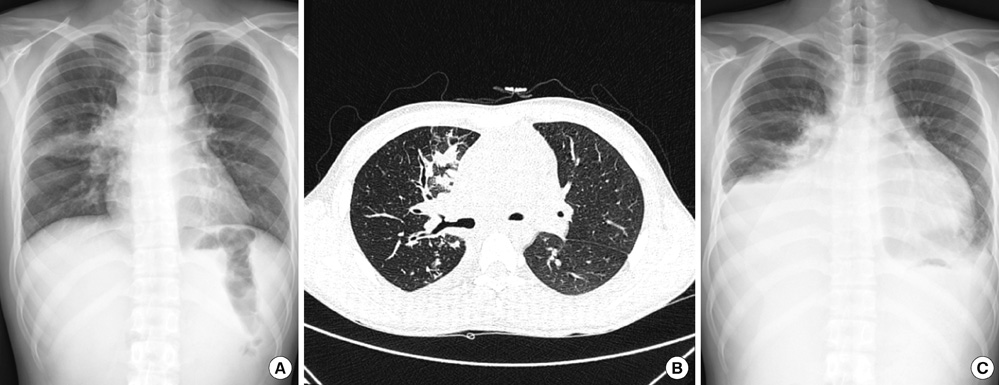
Fig. 1 Radiologic findings of the chest. (A) Haziness in right upper and middle lung was noted. (B) Consolidation, micronodules, and branching structures were found in the right lung, and lymph node enlargements were noted in both hilum. (C) Aggravated haziness in the right lung and newly appeared consolidation in the right lower lung were found on 7th hospital day.
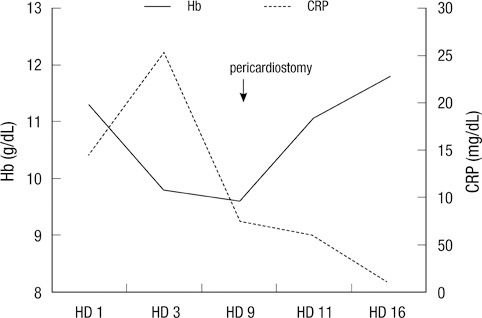
Fig. 2 Hemoglobin (Hb) was decreased gradually since admission till the 9th hospital day (HD), when pericardiostomy was performed. C-reactive protein (CRP) increased initially and then decreased. After pericardiostomy, hemoglobin increased till discharge and CRP also decreased to normal at discharge.
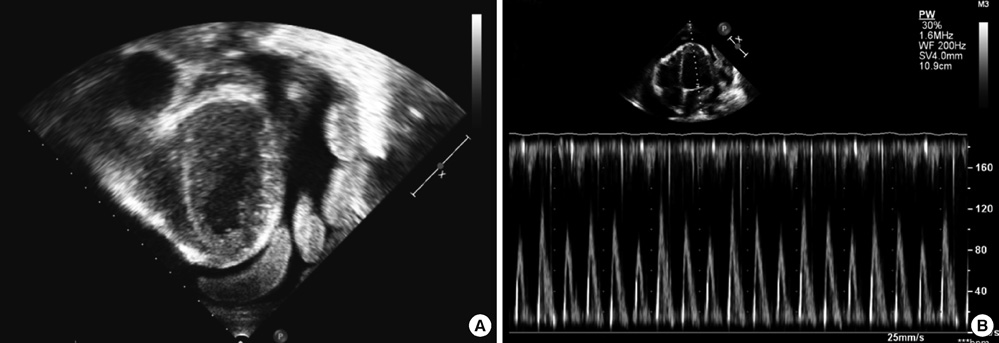
Fig. 3 Echocardiographic findings. (A) Free floating multiple round discoid echogenic masses in the large amount of pericardial effusion, the thickened pericardium and shaggy echo-dense appearance surrounding the epicardium in subcostal view, and (B) marked variation in mitral inflow Doppler pattern.

Fig. 4 Gross specimens obtained from pericardial space.
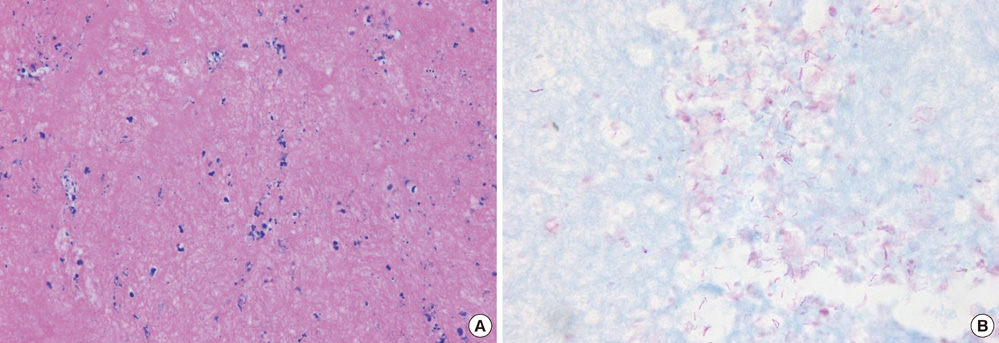
Fig. 5 Microscopic finding. (A) A pink, amorphous meshwork of threads admixed with degenerated red blood cells and leukocytes (H&E stain, × 400). (B) Numerous acid-fast bacilli (Ziehl-Neelsen stain, × 1,000).
Reference
-
1. Fowler NO. Tuberculous pericarditis. JAMA. 1991. 266:99–103.2. Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005. 112:3608–3616.3. Liu PY, Li YH, Tsai WC, Tsai LM, Chao TH, Yung YJ, Chen JH. Usefulness of echocardiographic intrapericardial abnormalities in the diagnosis of tuberculous pericardial effusion. Am J Cardiol. 2001. 87:1133–1135.4. Lin JH, Chen SJ, Wu MH, Lee PI, Chang CI. Fibrinofibrous pericarditis mimicking a pericardial tumor. J Formos Med Assoc. 2000. 99:59–61.5. Massoure PL, Boddaert G, Caumes JL, Gaillard PE, Lions C, Grassin F. Porridge-like tuberculous cardiac tamponade: treatment difficulties in the Horn of Africa. Gen Thorac Cardiovasc Surg. 2010. 58:276–278.6. Tirilomis T, Unverdorben S, von der Emde J. Pericardectomy for chronic constrictive pericarditis: risks and outcome. Eur J Cardiothorac Surg. 1994. 8:487–492.7. Bolt RJ, Rammeloo LA, van Furth AM, van Well GT. A 15-year-old girl with a large pericardial effusion. Eur J Pediatr. 2008. 167:811–812.8. Trautner BW, Darouiche RO. Tuberculous pericarditis: optimal diagnosis and management. Clin Infect Dis. 2001. 33:954–961.9. Blumberg HM, Burman WJ, Chaisson RE, Daley CL, Etkind SC, Friedman LN, Fujiwara P, Grzemska M, Hopewell PC, Iseman MD, Jasmer RM, Koppaka V, Menzies RI, O'Brien RJ, Reves RR, Reichman LB, Simone PM, Starke JR, Vernon AA. American Thoracic Society/Centers for Disease Control and Prevention and Infectious Diseases Society. American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America: treatment of tuberculosis. Am J Respir Crit Care Med. 2003. 167:603–662.10. Strang JI, Gibson DG, Nunn AJ, Kakaza HH, Girling DJ, Fox W. Controlled trial of prednisolone as adjuvant in treatment of tuberculous constrictive pericarditis in Transkei. Lancet. 1987. 2:1418–1422.11. Strang JI, Gibson DG, Mitchison DA, Girling DJ, Kakaza HH, Allen BW, Evans DJ, Nunn AJ, Fox W. Controlled clinical trial of complete open surgical drainage and of prednisolone in treatment of tuberculous pericardial effusion in Transkei. Lancet. 1988. 2:759–764.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of tuberculous pericarditis presenting as pericardial mass compressing pulmonary artery
- The Usefulness of Pericardial Biopsy to Evaluate the Causes of Pericardial Disease
- A Case of Tuberculous Pericarditis Diagnosed by Increased ADA Activity in Pericardial Fluid
- A Case of Constrictive Pericarditis with Localized Pericardial Effusion Simulating a Cystic Mass
- Tuberculous Pericarditis Mimicking a Malignant Pericardial Tumor: A Case Report
