Yonsei Med J.
2011 Mar;52(2):276-281. 10.3349/ymj.2011.52.2.276.
Utility of Procalcitonin as an Early Diagnostic Marker of Bacteremia in Patients with Acute Fever
- Affiliations
-
- 1Department of Laboratory Medicine, Kyung Hee University Hospital at Gandong, Seoul, Korea.
- 2Department of Laboratory Medicine, Kyung Hee University Medical Center, Kyung Hee University School of Medicine, Seoul, Korea. leehejo@khmc.or.kr
- KMID: 1779663
- DOI: http://doi.org/10.3349/ymj.2011.52.2.276
Abstract
- PURPOSE
Procalcitonin (PCT) is a current, frequently used marker for severe bacterial infection. The aim of this study was to assess the ability of PCT levels to differentiate bacteremic from nonbacteremic patients with fever. We assessed whether PCT level could be used to accurately rule out a diagnosis of bacteremia.
MATERIALS AND METHODS
Serum samples and blood culture were obtained from patients with fever between August 2008 and April 2009. PCT was analyzed using a VIDAS(R) B.R.A.H.M.S PCT assay. We reviewed the final diagnosis and patient histories, including clinical presentation and antibiotic treatment.
RESULTS
A total of 300 patients with fevers were enrolled in this study: 58 with bacteremia (positive blood culture) (group I); 137 with local infection (group II); 90 with other diseases (group III); and 15 with fevers of unknown origin (group IV). PCT levels were significantly higher in patients with bacteremia than in those with non-bacteremia (11.9 +/- 25.1 and 2.5 +/- 14.7 ng/mL, respectively, p < 0.001). The sensitivity and specificity were 74.2% and 70.1%, respectively, at a cut-off value of 0.5 ng/mL. A serum PCT level of < 0.4 ng/mL accurately rules out diagnosis of bacteremia.
CONCLUSION
In febrile patients, elevated PCT may help predict bacteremia; furthermore, low PCT levels were helpful for ruling out bacteremia as a diagnosis. Therefore, PCT assessment could help physicians limit the number of prescriptions for antibiotics.
Keyword
MeSH Terms
Figure
-
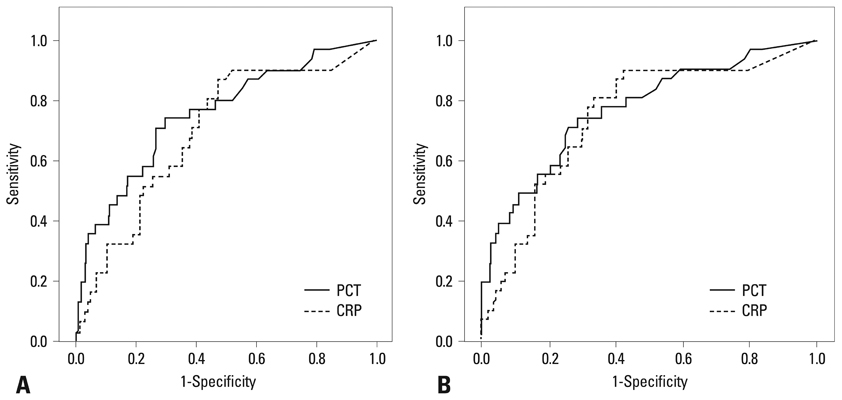
Fig. 1 (A) Receiver operator characteristic curve demonstrating sensitivity as a function of one-specificity for discriminating patients with blood culture positivity based on procalcitonin (PCT) and C-reactive protein (CRP) levels. PCT and CRP had areas under the receiver operator characteristic curve of 0.753 and 0.696, respectively. (B) Receiver operator characteristic curve demonstrating sensitivity as a function of one-specificity for discriminating patients with bacteremia from patients with localized infection based on PCT and CRP. PCT and CRP had areas under the receiver operator characteristic curve of 0.769 and 0.746, respectively.
Reference
-
1. Parrillo JE. Pathogenetic mechanisms of septic shock. N Engl J Med. 1993. 328:1471–1477.
Article2. Mitaka C. Clinical laboratory differentiation of infectious versus non-infectious systemic inflammatory response syndrome. Clin Chim Acta. 2005. 351:17–29.
Article3. Reimer LG, Wilson ML, Weinstein MP. Update on detection of bacteremia and fungemia. Clin Microbiol Rev. 1997. 10:444–465.
Article4. Jacobs JW, Lund PK, Potts JT Jr, Bell NH, Habener JF. Procalcitonin is a glycoprotein. J Biol Chem. 1981. 256:2803–2807.
Article5. Reinhart K, Karzai W, Meisner M. Procalcitonin as a marker of the systemic inflammatory response to infection. Intensive Care Med. 2000. 26:1193–1200.
Article6. Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 1993. 341:515–518.
Article7. Brunkhorst FM, Wegscheider K, Forycki ZF, Brunkhorst R. Procalcitonin for early diagnosis and differentiation of SIRS, sepsis, severe sepsis, and septic shock. Intensive Care Med. 2000. 26:Suppl 2. S148–S152.
Article8. Endo S, Aikawa N, Fujishima S, Sekine I, Kogawa K, Yamamoto Y, et al. Usefulness of procalcitonin serum level for the discrimination of severe sepsis from sepsis: a multicenter prospective study. J Infect Chemother. 2008. 14:244–249.
Article9. Harris KR, Digard NJ, Lee HA. Serum C-reactive protein. A useful and economical marker of immune activation in renal transplantation. Transplantation. 1996. 61:1593–1600.10. Jongwutiwes U, Suitharak K, Tiengrim S, Thamlikitkul V. Serum procalcitonin in diagnosis of bacteremia. J Med Assoc Thai. 2009. 92:Suppl 2. S79–S87.11. Luzzani A, Polati E, Dorizzi R, Rungatscher A, Pavan R, Merlini A. Comparison of procalcitonin and C-reactive protein as markers of sepsis. Crit Care Med. 2003. 31:1737–1741.
Article12. Chirouze C, Schuhmacher H, Rabaud C, Gil H, Khayat N, Estavoyer JM, et al. Low serum procalcitonin level accurately predicts the absence of bacteremia in adult patients with acute fever. Clin Infect Dis. 2002. 35:156–161.
Article13. Rowther FB, Rodrigues CS, Deshmukh MS, Kapadia FN, Hegde A, Mehta AP, et al. Prospective comparison of eubacterial PCR and measurement of procalcitonin levels with blood culture for diagnosing septicemia in intensive care unit patients. J Clin Microbiol. 2009. 47:2964–2969.
Article14. Bates DW, Sands K, Miller E, Lanken PN, Hibberd PL, Graman PS, et al. Academic Medical Center Consortium Sepsis Project Working Group. Predicting bacteremia in patients with sepsis syndrome. J Infect Dis. 1997. 176:1538–1551.
Article15. Müller B, Becker KL, Schachinger H, Rickenbacher PR, Huber PR, Zimmerli W, et al. Calcitonin precursors are reliable markers of sepsis in a medical intensive care unit. Crit Care Med. 2000. 28:977–983.
Article16. Liaudat S, Dayer E, Praz G, Bille J, Troillet N. Usefulness of procalcitonin serum level for the diagnosis of bacteremia. Eur J Clin Microbiol Infect Dis. 2001. 20:524–527.
Article17. Bossink AW, Groeneveld AB, Thijs LG. Prediction of microbial infection and mortality in medical patients with fever: plasma procalcitonin, neutrophilic elastase-alpha1-antitrypsin, and lactoferrin compared with clinical variables. Clin Infect Dis. 1999. 29:398–407.
Article18. Charles PE, Ladoire S, Aho S, Quenot JP, Doise JM, Prin S, et al. Serum procalcitonin elevation in critically ill patients at the onset of bacteremia caused by either Gram negative or Gram positive bacteria. BMC Infect Dis. 2008. 8:38.
Article19. Becker KL, Snider R, Nylen ES. Procalcitonin assay in systemic inflammation, infection, and sepsis: clinical utility and limitations. Crit Care Med. 2008. 36:941–952.
Article20. Hur M, Moon HW, Yun YM, Kim KH, Kim HS, Lee KM. [Comparison of diagnostic utility between procalcitonin and C-reactive protein for the patients with blood culture-positive sepsis]. Korean J Lab Med. 2009. 29:529–535.
Article21. Schuttrumpf S, Binder L, Hagemann T, Berkovic D, Trumper L, Binder C. Utility of procalcitonin concentration in the evaluation of patients with malignant diseases and elevated C-reactive protein plasma concentrations. Clin Infect Dis. 2006. 43:468–473.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictive value of procalcitonin for bacteremia in patients with pneumonia in the emergency department
- Clinical Usefulness of Procalcitonin as a Predictive Marker in Accordance with the Severity of Female Patients with Uncomplicated Acute Pyelonephritis
- The Usefulness of Procalcitonin and C-Reactive Protein as Early Diagnostic Markers of Bacteremia in Cancer Patients with Febrile Neutropenia
- Comparison of the diagnostic performance of initial serum procalcitonin, lactate, and C-reactive protein for predicting bacteremia in female patients with acute pyelonephritis
- Predictive Value of Serum Procalcitonin in Urinary Tract Infection Patients with Bacteremia
